
Kein Folientitel - PowerPoint PPT Presentation
1 / 1
Title:
Kein Folientitel
Description:
Functional Late Potential during Accelerated Heart Rate with Transesophageal Atrial Pacing ... For transesophageal atrial pacing with different electrodes, we used the ... – PowerPoint PPT presentation
Number of Views:48
Avg rating:3.0/5.0
Title: Kein Folientitel
1
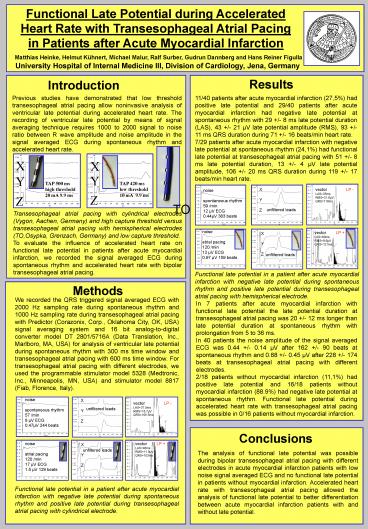
Functional Late Potential during Accelerated
Heart Rate with Transesophageal Atrial Pacing in
Patients after Acute Myocardial Infarction
Matthias Heinke, Helmut Kühnert, Michael Malur,
Ralf Surber, Gudrun Dannberg and Hans Reiner
Figulla
University Hospital of Internal Medicine III,
Division of Cardiology, Jena, Germany
Results
Introduction
Previous studies have demonstrated that low
threshold transesophageal atrial pacing allow
noninvasive analysis of ventricular late
potential during accelerated heart rate. The
recording of ventricular late potential by means
of signal averaging technique requires 1000 to
2000 signal to noise ratio between R wave
amplitude and noise amplitude in the signal
averaged ECG during spontaneous rhythm and
accelerated heart rate.
11/40 patients after acute myocardial infarction
(27,5) had positive late potential and 29/40
patients after acute myocardial infarction had
negative late potential at spontaneous rhythm
with 29 /- 8 ms late potential duration (LAS),
43 /- 21 µV late potential amplitude (RMS), 93
/- 11 ms QRS duration during 71 /- 16 beats/min
heart rate. 7/29 patients after acute myocardial
infarction with negative late potential at
spontaneous rhythm (24,1) had functional late
potential at transesophageal atrial pacing with
51 /- 8 ms late potential duration, 13 /- 4 µV
late potential amplitude, 106 /- 20 ms QRS
duration during 119 /- 17 beats/min heart rate.
X
X
Y
Y
TAP 500 ms high threshold 20 mA 9.9 ms
TAP 420 ms low threshold 10 mA 9.9 ms
X Y Z
vector LP - LAS35ms
RMS21.6µV QRS118ms
noise spontaneous rhythm 59 /min 12 µV
ECG 0.44µV 383 beats
Z
Z
TO
unfiltered leads
Transesophageal atrial pacing with cylindrical
electrodes (Vygon, Aachen, Germany) and high
capture threshold versus transesophageal atrial
pacing with hemispherical electrodes (TO,Osypka,
Grenzach, Germany) and low capture threshold. To
evaluate the influence of accelerated heart rate
on functional late potential in patients after
acute myocardial infarction, we recorded the
signal averaged ECG during spontaneous rhythm and
accelerated heart rate with bipolar
transesophageal atrial pacing.
noise atrial pacing 120 /min 12 µV ECG 0.97 µV
159 beats
vector LP LAS60ms RMS9.6µV
QRS121ms
X Y Z
unfiltered leads
Functional late potential in a patient after
acute myocardial infarction with negative late
potential during spontaneous rhythm and positive
late potential during transesophageal atrial
pacing with hemispherical electrode.
Methods
We recorded the QRS triggered signal averaged ECG
with 2000 Hz sampling rate during spontaneous
rhythm and 1000 Hz sampling rate during
transesophageal atrial pacing with Predictor
(Corazonix, Corp., Oklahoma City, OK, USA) signal
averaging system and 16 bit analog-to-digital
converter model DT 2801/5716A (Data Translation,
Inc., Marlboro, MA, USA) for analysis of
ventricular late potential during spontaneous
rhythm with 300 ms time window and
transesophageal atrial pacing with 600 ms time
window. For transesophageal atrial pacing with
different electrodes, we used the programmable
stimulator model 5328 (Medtronic, Inc.,
Minneapolis, MN, USA) and stimulator model 8817
(Fiab, Florence, Italy).
In 7 patients after acute myocardial infarction
with functional late potential the late potential
duration at transesophageal atrial pacing was 20
/- 12 ms longer than late potential duration at
spontaneous rhythm with prolongation from 5 to 36
ms. In 40 patients the noise amplitude of the
signal averaged ECG was 0.44 /- 0.14 µV after
162 /- 90 beats at spontaneous rhythm and 0.88
/- 0.45 µV after 228 /- 174 beats at
transesophageal atrial pacing with different
electrodes. 2/18 patients without myocardial
infarction (11,1) had positive late potential
and 16/18 patients without myocardial infarction
(88.9) had negative late potential at
spontaneous rhythm. Functional late potential
during accelerated heart rate with
transesophageal atrial pacing was possible in
0/16 patients without myocardial infarction.
noise spontaneous rhythm 57 /min 8 µV ECG 0.47µV
244 beats
X Y Z
vector LP - LAS37.5ms
RMS18.7µV QRS105.5ms
unfiltered leads
Conclusions
noise atrial pacing 120 /min 17 µV ECG 1.5 µV
129 beats
vector LP LAS46ms RMS11.9µV
QRS103ms
X Y Z
unfiltered leads
The analysis of functional late potential was
possible during bipolar transesophageal atrial
pacing with different electrodes in acute
myocardial infarction patients with low noise
signal averaged ECG and no functional late
potential in patients without myocardial
infarction. Accelerated heart rate with
transesophageal atrial pacing allowed the
analysis of functional late potential to better
differentiation between acute myocardial
infarction patients with and without late
potential.
Functional late potential in a patient after
acute myocardial infarction with negative late
potential during spontaneous rhythm and positive
late potential during transesophageal atrial
pacing with cylindrical electrode.
Recommended
CrystalGraphics Presentations





























