
Pituitary gland PowerPoint PPT Presentation
1 / 57
Title: Pituitary gland
1
Pituitary gland
2
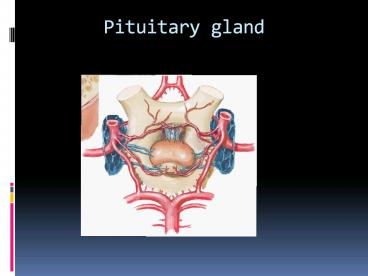
Gross anatomy of the pituitary gland
- The average weight of the pituitary gland at
birth is about 100 mg. Rapid growth occurs in
childhood, followed by slower growth until the
adult weight (approximately 500600 mg) is
attained in the latter part of the second decade.
The adult hypophysis measures approximately 10 mm
in length, 10 to 15 mm in width, and about 5 mm
in height
3
- Although the adult hypophysis typically measures
less than 1 cm in its greatest dimension and
weighs less than 1 g, its small size gives a
wrong idea about its importance and complexity - Embryogenesis of the pituitary gland
- The pituitary gland originates from two discrete
parts of the developing embryo ,(neural
epithelial) - The ant. Lobe develop from the roof of the
mouth(epith.)and called adenohypophysis - The post. Lobe develop from the
brain(neural)called neurohypophysis
4
- On average, the female gland is almost 20
heavier than the male gland primarily because of
relative di?erences in the size of the pars
distalis(adenohypophysis). - Furthermore, the weight of the gland increases
by 12 to 100 during pregnancy because of
enlargement of the pars distalis. - the size of the pars nervosa remains relatively
constant. - The volume of the pituitary gland decreases with
aging
5
(No Transcript)
6
(No Transcript)
7
- The pituitary gland derives its blood supply from
two groups of arteries. The superior hypophyseal
artery (SHA) primarily supplies the anterior
lobe, whereas the inferior hypophyseal artery
(IHA) is primarily related to the pars nervosa.
The SHA can arise from the supraclinoid portion
of the internal carotid artery (ICA) or from the
posterior communicating artery, whereas the IHA
arises from the meningohypophyseal trunk, a
branch of the cavernous segment of the ICA
8
The oculomotor nerve, trochlear nerve, and ?rst
two divisions of the trigeminal nerve are
embedded in the lateral wall of the cavernous
sinus, lying between the endothelial lining and
the dura mater, whereas the abducens nerve is
contained within the sinus itself
9
Pituitary tumors
10
Classificationsa. classification of pit.tumors
and tumor like conditions
- 1.tumors derived from adenohypophyseal
cells(adenoma, carcinoma) - 2.other primary tumors of sella
turcica.(angioma,craniopharyngioma,meningioma,opti
c nerve glioma - 3.metastatic tumors
- 4.tumor like conditions(abscess)
11
craniophryngioma
- Arise from anterior superior margin of pituitary
gland. - Lined by stratified squamouse epithelium
- All CP had solid and cyctic part,contain
cholestrol crystal (machine oil) - CP donot undergo malignant degeneration but
malignant behaviour,difficult cure (C.P adherant
to the major art. At the base of the brain(int.
carotid)
12
(No Transcript)
13
craniophryngioma
- Calcification in plain x ray
- 54 in childhood ,20, in adult ,
- 2.5 -4 of all brain tumor
- 9 of children brain tu.
- ,peak incidence age 5-10 year
- 55-85 five years survival rate
- 5-10- mortality due to hypothalamic injurey
- High recurrence rate in 1st 1-3 years
14
Signs symptoms
- Symptoms
- Headache,nausea vomiting,visual loss, short
- stature,mental problems,diplopia
- Signs
- Papilledema ,visual defect,endocrine
dysfunction,cranial nerve palsy,psychatric
abnormality
15
Management
- Diagnosis
- Plain x-ray, C.T , M.R.I, endocrine assessment
- Treatment
- Surgery(hydrocephalus,cyst drainage)
- Medical replacement(steroids,A.D.H replacement
with fluid) - Radiotherapy(better results in children than
adults)
16
Treatment of hydrocephalus
17
Ommaya reservior
18
Radiotherapy
- Linear accelerator
- Gamma knife radiosurgery
19
Pituitary adenoma
20
b.classification of pituitary adenomas according
to endocrine function
- -SECRETORY
- 1.prolactinoma
- 2.GH adenoma
- 3.ACTH adenoma
- 4.FSH/LH adenoma
- 5.T.S.H adenoma
- 6.plurihormonal adenoma(more than 1 hormone
secretion - -ADENOMA WITH NO APPERANT HORMONAL FUNCTION
21
c. Classification according to size on
radiographic appearance
- Grade-0 intrapit. Adenoma ,diam.less than 1
cm,normal sella - Grade-1 intrapit.ad.,diam.less than 1 cm,focal
bulging or minor changes in sellar shape - Grade-2 intrasellar adenoma,diam. More than 1
cm,enlarge sella, no erosion - Grade-3 diffuse ad.,diam more than 1 cm,enlarge
sella, localized erosion - Grade-4 invasive ad.,diam more than1 cm,extensive
destruction of bony struc.(gohst sella)
22
Adenoma
- Arise from adenohypophyseal cells
- 10-15 of intracranial tu.
- Benign tu. Mostly,slow-growing
- Adenoma with no apparent hor. Func.(20)
- Secretory adenoma(prolactinoma,GH,TSH,ACTH,FSH/LH
adenoma
23
PROLACTINOMA
- Most common functional pituitary tu., accounting
for approximately 25 of all pit. Tu. 3 of all
intracranial tumors - Prolactin level elevated(200-300ng/ml) ,lower
levels may be found if there is other tumors
compressing the stalk and interrupt the flow of
inhibitory dopamine.
24
Clinical presentation
- Mass effect (visual field defect(bitemporal
hemianopia),impaired acuity,headache,rarely
3rd,4th,6th nerve palsies,hydrocephalus, other
endocrinological symp.) - women symptoms(primary or secondary amenorrhoea
and infertility, galactorrhoea) - Men symptoms(decreased libido,impotence,oligosperm
ia) - Hyperprolactinoma suppresses the hypothalamic
pituitary-gonadal axis) leading to hypogonadism
in both sexes
25
DIAGNOSIS
- Endocrine testing
- 1.fasting level of prolactine(gt150ng/ml indicate
that the cause pit.adenoma, if it gt1000ng/ml ,it
signify the invasiveness of tu. that extend to
cavernous sinus) - 2. other hormonal assessment(pit.-thyroid
,pit.-gonadal(FSH-LH,testosterone),pit-adrenal(a.m
cortisol),antidiuretic hor,(urine serum
electrolytes)
26
Neuroimaging studies
- C.T SCAN of sella with thin slices(1.5-2 mm)plus
contrast ,to exclude ac. Haemorrhage. - MRI of sellar parasellar(lt2.5mm slices)
- Cerebral angiography or MRI angio to exclude
aneurysms.
27
(No Transcript)
28
TREATMENTMode of treatment depend on
- 1.size of tumor
- 2.the level of serum prolactin.
- 3.the patient age overall health.
- 4.The patients tolerance of or compliance with
medical therapy. - 5.the patient desires fertility.
- 6.surgical risk factors
29
Indications of surgical treatment of prolactinoma
- 1.Non invasive tu. With prolactine
level(150-500ng/ml) and patient not wish to take
long term medications. - 2.A woman with non invasive tu.,prl. (lt500
ng/ml),who desires pregnancy. - 3. A Woman with macroprolactinoma who desire
pregnancy. - 4.Macroprolactinoma with s.prolactingt500ng/ml
- 5.Pituitary apoplexy as a complication of
prolactinomagt - 6.A prolactinoma in pregnant patient causing mass
effect( visual loss) - 7.A prolactinom that is not respond to medical
treatment - 8.A recurrent prolactinoma
30
SURGICAL TREATMENT
- Craniotomy (rt. Frontal)
- Trans-sphenoidal transnasal approach
31
craniotomy
32
transsphenoidal
33
(No Transcript)
34
COMPLICATIONS OF TRANS-SPHENOIDAL
- 1.C.S.F leak
- 2.Meningitis
- 3.Hypopituitarism Diabetes insipidus
- 4.pneumocephalus
35
RADIOTHERAPY
- 1.conventional external radiation
- Adverse effect(hypopituitarysm, optic nerve or
chiasmal injury,brain radionecrosis,carcinogenesis
)
36
- 2.stereotactic radiosurgery (GAMMA KNIFE
RADIOSURGERY). - Indication(microadenoma or macroadenomalt5 cm)
37
Gamma knife
38
Pituitary apoplexy
- Acute haemmorrhagic necrosis of a pituitary
adenomaadjacent pituitary tiss. - Predisposing factorspregnency,endocrinologic
manipulations(estrogen adminstration,bromocriptine
medication),H.injury,chronic coughsneezing,antic
oagulant drugs,cerebral angio.,radiotherapy
39
Symptoms signs
- Headache,nausea vomiting, diplopiavisual
impairment, compression of cranial n.s in one or
both cavernous sinuses,ophthalmoplegia, meningeal
irritation,photophobia - Diagnosis(MRA,ANGIO,CT,CLINICAL)
- Treatment
- surgery
40
(No Transcript)
41
(No Transcript)
42
Acromegaly
43
The aims of acromegaly treatment
- (1) to control clinical signs while preserving
pituitary function with as minimal adverse
effects as possible. - (2) to normalize excessive growth hormone (GH)
and IGF-1 secretion as quickly as possible,
thereby achieving biochemical control - (3) to avoid the expansion of the tumor volume
and if possible reduce tumor size in order to
relieve any symptom due to tumor mass.
44
TREATMENT ALGORITHM
Neurosurgery 56877-885, 2005)SRLSsomatostatin
receptor ligand ,DAdopamine agonist)
45
Indications for surgery include
- active acromegaly
- visual loss and other forms of mass effect
- pituitary tumor apoplexy
- failure of other therapies (medical, radiation).
46
- visual compromise develops quite slowly and
gradually - surgical decompression of visual pathways is
usually recommended unless the compression can be
resolved by medical treatment. - Undisputedly, the most rapid and reliable relief
from optic nerve and chiasmal compression is
being achieved by surgery, which is particularly
appreciated if severe loss of vision occurred
acutely, as in pituitary apoplexy
47
- Hormonal oversecretion for patients with
secretory pituitary adenoma increasing the
morbidity and mortality. - Clinical diagnosis of these diseases is
generally considered an indication for surgery. - Because surgery is still generally considered
the most rapidly acting and cheapest long-term
solution for most patients.
48
- recent data suggest that hypopituitarism can also
be considered an indication for surgery since
pituitary function may be improved following
decompression of the gland by selective tumour
resection
49
- A conservative approach is usually recommended in
incidentally detected lesions, which became more
frequent with the widespread availability of MR
imaging.
BUT the progression of a tumour, which is
clearly documented in the MR, is another
indication to surgically attack a lesion that has
already shown an increase in size.
50
Re-operations should be strongly considered if
- a resectable lesion has not been excised
satisfactorily by the primary intervention - patients with recurrent disease, if adjunctive
medical or radiation therapy failed to achieve
control of the adenoma - in symptomatic progressions of residual tumours.
It seems easier for an expert neurosurgeon with
an excellent success and a low complication rate
to recommend an operation for a pituitary tumour
51
Radiotherapy
- Stereotactic radiosurgery
- Conventional radiotherapy
- Remission rate (50-60)
- Time of remission delayed by several years(10y).
- Propsed for patients with aggressive adenoma when
surgery cannot allow biochemical control. - Hypopituitarism increases with time
(50-80),also its more with previosly altered
pit. Function(by surgery)
- Remission rate(17-96)
- faster growth hormone hypersecretion decline.(2y)
- requires a well defined target volume.
- be used as an alternative primary treatment to
surgery. - Hypopituitarism(0-33)
52
- Optic neuropathy, radionecrosis, vascular injury
- were much lower in gamma knife than
- conventional radiothearapy
53
(No Transcript)
54
(No Transcript)
55
Pre.
56
Post
57
Post medical.
Recommended
