
The Adrenal Gland PowerPoint PPT Presentation
1 / 102
Title: The Adrenal Gland
1
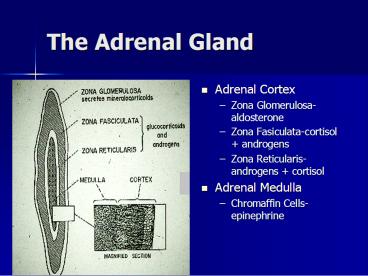
The Adrenal Gland
- Adrenal Cortex
- Zona Glomerulosa-aldosterone
- Zona Fasiculata-cortisol androgens
- Zona Reticularis-androgens cortisol
- Adrenal Medulla
- Chromaffin Cells-epinephrine
2
Glucocorticoids
- Cortisol
- Corticosterone
- Deoxycorticosterone
- 11-deoxycortisol
- others
3
Effects of Glucocorticoids
- Carbohydrate Metabolism
- Gluconeogenesis
- Decreased Glucose Utilization
- Increased Glycogen Stores
- Protein
- Catabolic
4
Effects of Glucocorticoids
- Lipid
- Decreased Lipogenesis
- Stimulated Lipolysis
- Change in distribution
- Electrolytes
- Increases Ca and Phos excretion
- Decreased Ca Absorption
- Weak mineralocorticoid action
5
Effects of Glucocorticoids
- Water Homeostasis
- increased GFR
- inhibitory to ADH
- Circulation
- Permissive effect for norepinephrine
- Blood
- Increased PMNs, Platelets, RBCs
- Decreased Eosinophils and Lymphocytes
6
Effects of Glucocorticoids
- Connective Tissue
- Decreased Fibroblast Proliferation
- Collagen Catabolism
- Gastrointestinal Tract
- Increased Gastrin, Gastric Acid, Pepsin
- Decreased Gastric Mucus Content Viscosity
- Decreased Gastric Mucosal Cell Proliferation
7
Effects of Glucocorticoids
- Liver
- Increased Glycogen
- Increased Gluconeogenesis
- Induction of Enzymes
- Pancreas
- Anti-inflammatory
- Stabilize membrane (Cellular, Lysosomal)
- Inhibits Fibroblast Proliferation
- Inhibit WBC migration/phagocytosis
8
Effects of Glucocorticoids
- Immunosuppressive
- Effect on WBCs, Macrophages
- Effect on Lymphocytes
- Appetite Stimulation
- CNS effect
- Diabetes Mellitus
- Neurologic Effects
9
Therapeutic Use of Corticosteroids
- Allergic conditions
- Autoimmune disorders
- Pruritus with self-mutilation
- Destructive inflammation
- CNS trauma, shock
- Hypoglycemia, hypercalcemia
- Cancer chemotherapy
10
Complications of Corticosteroid Therapy
- Iatrogenic Cushings
- Adrenocortical Suppression
- Immunosuppression
- Steroid Hepatopathy
- Wound Dehiscence
- Diabetes Mellitus
- GI Ulcers
11
Complications of Corticosteroid Therapy
- Pancreatitis
- Muscle Weakness
- Osteoporosis
- Growth Retardation
- May worsen many diseases
- arthritis
- demodex
- Renal failure
12
(No Transcript)
13
Duration Varies with Form
- Succinate - hours
- Unesterified - hours
- Acetate - days to months
- Pivalate - months
14
Glucocorticoid Dosages
- Maintenance (physiological)
- Hydrocortisone 0.1-0.5 mg/lb/day
- Prednisolone 0.02-0.1 mg/lb/day
- Anti-inflammatory
- Prednisolone 0.25-0.5 mg/lb/day
- Dexamethasone 0.05 mg/lb/day
15
Anti-inflammatory Therapy
- Loading dose for 5-7 days
- dogs 0.5 mg/lb/day
- cats 1-2 mg/lb/day
- Maintenance
- dogs 0.25-0.5 mg/lb q 48 hrs
- cats 1 mg/lb q 48 hrs
16
Gluocorticoids in Therapy
- Immunosuppressive (dogs cats 2X)
- Prednisone 1-2 mg/lb/day
- Dexamethasone 0.1-0.2 mg/lb/day
- Shock and CNS trauma
- Prednisolone 5-25 mg/lb/day
- Dexamethasone 1-5 mg/lb/day
17
Hyperadrenocorticism
- Cushings Syndrome
- Cushings Disease (PDH)
- Hyperglucocorticoidism
18
Forms of Hyperadrenocorticism
- Bilateral Adrenocortical Hyperplasia
(Pituitary-Dependent Hyperadrenocorticism, PDH) - Adrenal Tumor (functional)
- Iatrogenic
19
Pituitary Secretion of ACTH
- Pars Distalis
- ACTH secretion controlled by CRF via
hypophyseal-pituitary portal system - Pars Intermedius
- A cell pars intermedia MSH and B cell pars
intermedia ACTH secretion controlled by
serotonergic and dopaminergic fibers
20
Bilateral Adrenocortical Hyperplasia(Pituitary
Dependent Hyperadrenocorticism)
- Functional Pituitary Tumor
- pars distalis or pars intermedia
- Boston Terriers and Boxers
- Idiopathic Adrenal Hyperplasia
- abnormalities in neuro-endocrine transmitters
- Norepinephrine, Serotonin, Dopamine
- Most common in Dachshunds and poodles
- Ectopic ACTH-Producing Tumor
21
Adrenocortical Neoplasia(Adrenal Dependant
Hyperadrenocorticism)
- 10-20 of canine cases, 70 female
- Right Gland more often affected (77)
- Usually unilateral with atrophy of other
- Usually function independently of ACTH
- 60 Adenocarcinomas
- 40 Adenomas
22
Iatrogenic Canine Cushings Syndrome
- Exogenous glucocorticoids causing clinical signs
of cortisol excess - There is atrophy of the adrenal zona fasiculata
- Thus have adrenal suppression despite signs of
cortisol excess
23
Clinical Signs
- Polyuria
- Polydipsia
- Polyphagia
- Pendulous Abdomen
- Muscle weakness
- Lethargy
24
Dermatological Manifestations
- Alopecia
- Dermal Atrophy
- Hyperkeratosis, Comedones
- Increased bruising
- Hyperpigmentation
- Calcinosis cutis
- Poor wound healing
- Facial Dermatitis
25
(No Transcript)
26
(No Transcript)
27
(No Transcript)
28
- Steroid Hepatopathy
- Predisposition to Infections
- Reproductive Abnormalities
- Dystrophic calcification
- Osteoporosis
- Neurological Signs d/to pit. tumor
- Panting
- Obesity
- Thromboembolism (sudden death)
29
Possible Associated Syndromes
- Diabetes mellitus
- Pancreatitis
- Congestive Heart Failure
- Pulmonary Thromboembolism
- Pyelonephritis
- CNS Signs
30
Differential Diagnoses
- For PU/PD
- Chronic renal disease
- Liver disease
- Diabetes mellitus
- Diabetes insipidus
- Hyperthyroidism
- Electrolyte disorders
- Primary polydipsia (psychogenic)
- Etc.
31
Differential Diagnoses
- For dermatological signs
- Hypothyroidism
- Sex hormone imbalances
- Post-clipping alopecia
- Growth-hormone responsive dermatosis
- Alopecia X
- Demodecosis, dermatophytosis, etc.
32
Steps in Diagnosis
- Documentation of systemic effects associated with
high levels of glucocorticoids - Confirm diagnosis of hyperglucocorticoidism
- Determine etiology of hyperglucocorticoidism
33
Laboratory Evaluation
- Hemogram
- Stress Leukon
- Urinalysis
- Specific gravity
- ? Bacteriuria
34
Blood Chemistry
- Glucose
- Cholesterol
- Alanine transaminase
- Alkaline Phosphatase
- BUN
- Electrolytes
35
Other Tests
- Glucose Tolerance
- Blood Insulin
- Decreased total T3 T4
- Free T3 and T4 usually normal
- Endogenous TSH decreased
- Decreased serum phosphorus
- Elevated blood pressure
36
Radiology
- Hepatomegaly
- Carcinomas
- Osteoporosis
- Metastatic Mineralization
37
Abdominal Imaging
- Hepatomegaly
- Adrenal mass ? calcified
- Metastatic mineralization (e.g. renal)
- Ultrasonography can be very helpful in defining
the sizes of the adrenal glands and is used to
distinguish bilateral hyperplasia from adrenal
tumors
38
CT or MRI Scans
- Adrenal glands
- Hyperplasia
- Tumors
- Invasion into surrounding tissues
- Pituitary gland
- tumors
39
Liver Aspirates or Biopsies
- Ultrasound-guided or laparoscope
- Steroid hepatopathy
- Centrilobular vacuolation
- Glycogen accumulation
40
Exploratory
- Laproscope
- Laporatomy
- Visualize the adrenal glands
- Biopsy
- Removal a unilaterally enlarged gland
41
Adrenal Function Tests
- First step is to confirm an abnormality in
adrenal function, this confirms the diagnosis of
hyperglucocorticoidism
42
Measuring Plasma Cortisol
- EDTA
- Spin Immediately
- Freeze Plasma
- Methodology
- Fluorometric
- Competitive Protein Binding
- Radioimmunoassay
- ELISA
43
Adrenal Function Tests
- Resting plasma cortisol
- ACTH Stimulation Test
- 1 unit/lb ACTH GEL IM
- Pre and 2 hour post sample
- Or 5 ug/kg synthetic ACTH IV or IM
- Pre and 1 hour post sample
44
ACTH Stimulation Test Interpretation
- Normal
- pre 5-40 ng/ml or 15-110 nmol/L
- post 80-200 or 220-500 nmol/L
- PDH
- pre Normal or increased
- post 200 ng/ml or 600 nmol/L
45
ACTH StimulationTests Interpretation
- ADH
- pre normal or increased
- 50 have no increase, 50 have exaggerated
increase - Iatrogenic
- pre decrease
- post has no change
46
Adrenal Function Tests Interpretation
- Problems
- 10 of PDH do not have hyperplastic response and
some tumors do
47
Dexamethasone Suppression Tests
- Dexamethasone suppresses release of ACTH
resulting in decreased cortisol secretion - In PDH, low doses of DXMS do not suppress ACTH,
high doses do - Adrenal tumors function autonomously
48
(No Transcript)
49
Low Dose Dexamethasone Suppression Test
- To differentiate a dog with normal HPA axis
function from a dog with Cushings Syndrome - 0.01 mg/kg DXMS IV
- Pre, 3 hr and 8 hr post samples for cortisol
measurement
50
Low Dose Dexamethasone Suppression Test
Interpretation
- Normal HPA axis function
- Pre 15-110 nmol/L
- 3 and 8 hour post
- PDH (bilateral adrenal hyperplasia)
- Pre often 110 nmol/L
- 3 hr post maybe 50
of baseline ( transient ?) - 8 hr post 50 of baseline
51
Low Dose Dexamethasone Suppression Test
Interpretation
- Adrenal Tumors
- Pre often 110 nmol/L
- 3 and 8 hour post 50 of baseline
- Iatrogenic hyperglucocorticoidism
- This test is not indicated in diagnosis of
iatrogenic Cushings Syndrome
52
High Dose Dexamethasone Suppresssion Test
- This is done AFTER a diagnosis of
hyperadrenocorticism has been confirmed via an
ACTH stimulation test or a low dose dexamethasone
suppression test - 0.1 mg/kg dexamethasone IV
- Pre and 8 hour post samples
53
High Dose Dexamethasone Suppression Test
Interpretation
- Normal test not indicated
- Iatrogenic test not indicated
- PDH (bilateral adrenal hyperplasia)
- Pre often 110 nmol/L
- Post 50 suppression (usually
- Adrenal Tumor
- Pre often 110 nmol/L
- Post does NOT suppress to
54
Mega Dose Dexamethasone Suppression Test
- In past was advocated for identifying dogs with
pituitary tumors that were relatively refractory
to dexamethasone and only suppressed when given
very high doses (up to 25 of dogs with tumors of
pars intermedia) - 1 mg/kg IV with 0 and 8 hour post
- Interpretation same as high dose DST
55
Problems with Dexamethasone Suppression Tests
- Rate of metabolism of dexamethasone varies
between dogs and affects test results - Up to 25 of dogs with tumors of pars intermedia
do not suppress - Dogs with adrenal tumors may have fluctuations in
baseline cortisols that mimic suppression
56
(No Transcript)
57
(No Transcript)
58
Combination testing
- Some endocrinologists have recommended
combinations of an ACTH stimulation test and a
high dose dexamethasone suppression however these
often have confusing results and are not
recommended
59
Urine Cortisol Creatinine RatioJAVMA
200163-1641
- Normal mean 5.7
- 40 PDH dogs mean 337.6
- 23 other dogs with PU/PD mean 42.6
- Sensitive as screening test
- Not specific
- individual dogs overlapped in PDH and PU/PD gps)
60
Endogenous ACTH
- Elevated in PDH
- Suppressed with adrenal tumors and dogs with
iatrogenic hyperglucocorticoidism - ACTH is secreted episodically so wide normal
range and overlaps are seen - ACTH is not stable and requires special sample
handling
61
(No Transcript)
62
Examples of Test Results
63
Treatment
- General supportive care for any secondary
infections or diseases such as hypertension and
diabetes mellitus - Specific treatment of Cushings Syndrome depends
upon identification of the underlying cause (PDH,
adrenal tumor or iatrogenic)
64
Treatment Pituitary Dependent Hyperadrenocorticis
m
- Hypophysectomy
- requires surgical expertise or many
complications - Require glucocorticoids, thyroxine, ? ADH
- Bilateral Adrenalectomy
- Surgical complications may occur
- Paracostal approach preferred
- Require mineralcorticoids ? glucocorticoids
65
Lysodren (o,pDDD)
- Most common treatment of PDH
- Concentrated in adrenal cortex
- Selective necrosis of zona fasiculata and zona
reticularis - If overdose can also destroy the zona glomerulosa
66
Lysodren Induction
- Accurate Weight
- Baseline 24 hours water consumption
- Baseline eosinophil and lymphocyte number, Bun,
electrolytes
67
Lysodren Induction
- Give 25 mg/kg BID until
- Appetite decreases
- Decrease water consumption (
- Eosinophils 300/?l or Lymphs 1000 /?l
- 7-10 days (range 4-30)
- Minimal Response on ACTH Challenge
- Adverse signs
- Lysodren maintenance
- 25 mg/kg twice weekly
- (Sunday PM, Thursday AM)
68
Monitoring o,pDDD Therapy
- Clinical observations
- appetite, drinking, general attitude
- laboratory
- CBC, BUN, electrolytes, UA with culture
- q 1-3 months
- ACTH stimulation
- q month until stable
- q 3-6 months for life
69
Ideal ACTH Stimulation Results for Dogs on
o,pDDD Therapy
- Low normal resting cortisol
- Minimal response to ACTH
- post
70
Lysodren Maintenance
- Usually 25 mg/kg twice weekly
- Adjust based on ACTH response
- Often require increases in Lysodren dose during
the first year of treatment (have progressive
increases in ACTH) - Recheck ACTH response at end of a new induction
or one month after dosage change
71
Example Cases
- Dog with PDH has been on Lysodren 25 mg/kg twice
weekly - ACTH response test pre 220, post 660
- Would recommend repeating Lysodren induction,
e.g. 25 mg/kg BID for 5 days then recheck ACTH
response test - At recheck pre 80, post 60
- Resume 25 mg/kg twice weekly
72
Example Case
- Dog has been on Lysodren maintenance 25 mg/kg
twice weekly - ACTH response test pre 150, post 210
- Recommend increasing maintenance dose and recheck
ACTH response in one month - 37.5 mg/kg twice weekly (or 25 mg/kg three days
per week)
73
Example case
- Dog has been on maintenance Lysodren 25 mg/kg
twice weekly - ACTH response test pre 20, post 35
- Recommend stopping Lysodren for one month and
rechecking, if cortisol levels have increased
would then restart Lysodren at a lower dose (e.g.
25 mg/kg once weekly)
74
Client Education re Lysodren
- Lysodren is a very potent medication related to
DTT - Lysodren is very effective for the treatment of
Cushings Diseases but its use MUST be carefully
monitored - Veterinarian should be called anytime the dog has
a decrease in appetite or seems listless or has
any other symptoms of illness - Prednisolone is an antidote, owner should give
0.5 mg/kg if the dog shows listlessness or any
symptoms of illness or if known stress will be
occurring (grooming, travel, boarding, etc.)
75
Concurrent Cushings and Diabetes Mellitus
- Roughly regulate with insulin
- Induction dose 25 mg/kg o,pDDD per day
- Prednisolone 0.1 mg/kg given daily during
induction and for 3-5 days after cessation of
daily Lysodren - Maintenance 25 mg/kg o,pDDD twice weekly
- Expect dramatic decrease in insulin required
76
Alternate Medical Therapies
- Cyproheptadine (blocks serotonin)
- 0.05 mg/kg QID
- side effects hyperphagia, weight gain, vomiting,
diarrhea - Bromocriptine (dopamine agonist)
- 0.05-0.1 mg/kg/day bid
- Side effects anorexia, vomiting, behavioral
changes, depression
77
Alternate Medical Therapies
- Aminoglutethimide-blocks steroid synthesis
however only works short X - Metyrapone-blocks steroid synthesis
- 25 mg bid
- Trilostane-blocks steroid synthesis
- Early trials using 20-120 mg/dog look promising
- Mifepristone (RU486)-inhibits cortisol binding to
receptors - High levels of cortisol will override its
effectiveness
78
Ketoconazole
- Inhibits 11-hydroxylase and 14-demethylation
enzymes in steroid synthesis - May block steroid receptors
- Starting dose 10 mg/kg BID
- recheck ACTH stimulation in 10 days
- if cortisol 100 nmol/L increase to 15mg/kg BID
79
Ketoconazole Side Effects
- Anorexia
- discontinue for 24 hours
- Vomiting
- Hepatotoxicity
- monitor chemistry panels
- Lightening of the haircoat
80
Ketoconazole
- Advantages
- no danger of destroying the adrenal glands
- Also treats any secondary Malassezia infections
- Rapid decreases in serum cortisol
- Disadvantages
- Expensive
- Must be given BID
- Can cause anorexia, GI upsets, hepatic damage
81
L-Deprenyl (Anipryl)
- Irreversible inhibitor of monoamine oxidase type
B (increases CNS dopamine) - Is most effective in cases with tumors of pars
intermedia (approx 30 of canine pituitary
tumors) - Proposed to down regulate ACTH production
82
L-Deprenyl
- Is FDA approved for the treatment of canine PDH
- Evidence of effectiveness was based on owners
observations that treated dogs had more energy
(perhaps due to the drugs amphetamine activity) - No effect on serum cortisol level, liver enzymes,
etc.
83
L-Deprenyl
- Does not require monitoring of ACTH response
(does not decrease) - Side effects include vomiting, diarrhea,
restlessness, lethargy, salivation, anorexia,
deafness, pruritus, licking, shivering,
trembling, shaking, drug interactions with other
MOA inhibitors - ?????consider in very early cases, otherwise do
not recommend this drug as does not prevent
progression of disease in most dogs
84
Radiation Therapy for PDH
- Cobalt therapy
- reduces size of pituitary tumors
- may ameliorate neurologic signs
- Seldom decreases ACTH secretion
- No effect on adrenocortical hyperplasia
85
Surgery for Adrenal Tumors
- Adrenalectomy is treatment of choice
- 50 of tumors malignant and locally aggressive
- do CT scan or MRI to assess
- intra- and post-operative glucocorticoids
short-term minerolocorticoids as contralateral
gland atrophic
86
Lysodren for Adrenal Tumor
- Chemoablate the tumor
- 25 mg/kg BID for 14-30 days or until develop
complete adrenal insufficiency - Start Florinef at 0.1 mg/10kg SID to BID on day 7
of treatment - may need to also supplement with pred
87
Ketoconazole for Adrenal Tumor
- Blocks synthesis of cortisol
- 10-15 mg/kg BID for life
- No effect on the tumor,
- ameliorates clinical signs
88
Iatrogenic Cushings Disease
- Any or all of clinical and laboratory changes may
be present - Effects depend on type, dose, frequency and
duration of therapy - Diagnosis via ACTH challenge
- Crisis Treatment (following abrupt withdrawal)
- IV fluids
- Glucocorticoids
89
Iatrogenic Cushings Disease
- Maintenance during weaning off steroids
- Physiological replacement doses
- hydrocortisone 0.5-1 mg/kg/day
- prednisone 0.1-0.25 mg/kg e.o.d.
- Use ACTH Challenge to assess recovery
- Give 10X maintenance before stress
90
Iatrogenic Cushings Disease
- Prevention
- Use corticosteroids sparingly
- Use short acting forms
- Reserve long acting forms or DEPO for problems
that require only 1 or 2 doses
91
Feline Hyperadrenocorticism
92
Clinical Features
- Females predisposed (91)
- Middle-aged to older
- Truncal alopecia
- Hyperpigmentation
- Think skin
- Muscle wasting
- pendulous abdomen
93
Clinical Features
- Weight loss
- Polyphagia
- Diarrhea
- Infections
- Hepatomegaly
- PU/PD (late onset)
- Diabetes mellitus
94
Laboratory Finding
- Hyperglycemia
- Hypercholesterolemia
- Glucosuria
- Lymphopenia
- Eosinopenia
- Mature leukocytosis
- Increased SAP
95
Pituitary-Adrenal
- Function Tests
96
Low Dose Dexamethasone Suppression Test
- Normal cats will suppress cortisol levels by 50
following 0.01 mg/kg DXMS IV - Many cats with non-adrenal illnesses DO NOT
suppress cortisol levels by 50 following 0.01
mg/kg DXMS - Rules out normal cats, may not distinguish
between adrenal disease and other systemic
diseases causing PU/PD/PP, thin skin, etc.
97
High Dose Dexamethasone Suppression Test
- 0.1-1.0 mg/kg IV
- This is used as a SCREENING test for
hyperadrenocorticism in cats - Sample at 0 and 8 hours
- Normal cats and cats with non-adrenal illnesses
will have cortisol
98
Endogenous ACTH Response Test
- Normal range 20-100 pg/ml
- May be helpful in distinguishing between PDH and
adrenal tumors in cats - Adrenal tumors have low levels
- PDH is associated with high levels
- Overlaps do occur
99
Abdominal Ultrasonography
- Best method of differentiating PDH and adrenal
tumors in cats
100
Therapy
- o,pDDD not effective in decreasing cortisol
concentrations in cats - Ketoconazole not effective in decreasing
cortisol concentrations in cats - Metyrapone not effective in cats
- Cobalt Radiation may abalate pituitary tumor
without any effect on cortisol levels
101
Therapy
- Adrenalectomy
- Unilateral if adrenal tumor
- Bilateral for PDH
- Pre and post-surgery give glucocorticoids and
Florinef esp. if bilateral surgery to be done,
maintain on fluids, continue treatment of
diabetes (noting that insulin requirement likely
to drop)
102
Prognosis
- Guarded in cats due to high incidence of
complications relating to the Cushings disease
or to inability to manage post-operative
hypoadrenocorticism
Recommended
