
Pediatric Skin Disorders PowerPoint PPT Presentation
1 / 42
Title: Pediatric Skin Disorders
1
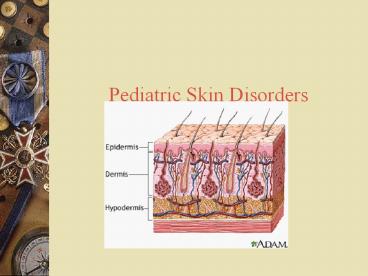
- Pediatric Skin Disorders
2
Compare skin differences
- Infant skin not mature at birth
- Adolescence sebaceous glands become enlarged
active.
3
Skin Assessment
- Assess history
- Assess exposure
- Assess character
- Assess sensation
4
Dermatitis
5
Dermatitis
- Inflammation of the skin that occurs in response
to contact with an allergen or irritant also
referred to as contact dermatitis
6
Dermatitis
- Common irritants
- Soap, fabric softeners, lotions, urine and
stool - ? Common allergens
- poison ivy, poison oak
- lanolin, latex, rubber
- nickel, fragrances
7
Dermatitis signs and symptoms
- Erythema
- Edema
- Pruritus
- Vesicles or bullae
- that rupture, ooze and crust
8
Dermatitis Treatment
- Medications
- Application of a corticosteroid topical agent
remind pt to continue use for 2-3 wks after signs
of healing - Application of protective barrier ointments
- Oatmeal baths, cool compresses
- Antihistamines given for sedative effect
9
Eczema
- Chronic superficial skin disorder characterized
by intense pruritis
10
Eczema signs and symptoms
- Erythematous patches with vesicles
- Pruritis
- Exudate and crusts
- Drying and scaling
- Lichenification
- (thickening of the skin)
11
Eczema, cont.
12
Goal of Treatment
- Hydrate the skin
13
Treatment of Eczema
- Emollients (creams which lubricate the skin)
- Oral antihistamines (control itching)
- Antibiotics (treat superinfections)
- Corticosteroids (anti-inflammatories)
- Immunomodulators (inhibit T lymphocyte
activation) - AVOID SOAPS!
14
Acne
15
Acne
- Inflammatory disease of the skin involving the
sebaceous glands and hair follicles. - Contributing factors include heredity,
hormonal influences and emotional stress
16
Acne Three main types
- Follicular plugs
- Pustular papules
- Cystic nodules
17
Patient teaching
- Do not pick! This increases the bacterial count
on the surface of the skin and opens lesions to
infection which worsens scarring - Remind patients that the treatment will not show
improvement until about 4-6 weeks but they must
consistently follow the regime set up by the
physician
18
Medical treatment for acne
- Topical (Benzoyl peroxide, Tretinoin (RetinA),
topical preferred to systemic however, both may
be needed - Oral Tetracycline, minocycline, erythromycin
estrogen for female pts., Accutane
19
Acne Nursing care
- Avoid picking and squeezing
- Use gentle skin cleansers
- Avoid use of astringents containing ETOH
- Avoid hats or abrasive rubbing of the skin
- Wash hands after handling greasy foods
- Limit use of petrolatum-based hair products hair
away from face - Use oil-free makeup, protections from windy, cold
weather - Continue therapy even when improved
20
Impetigo
- http//www.emedicine.com/emerg/topic283.htm
- Impetigo became infected
- Hemolytic Strep infection of the skin
- Incubation period is 2-5 days after contact
21
- Begins as a reddish macular rash, commonly seen
on face/extremities - Progresses to papular and vesicular rash that
oozes and forms a moist, honey colored crust.
Pruritis of skin - Common in 2-5 year age group
22
Therapeutic Management
- Apply moist soaks of Burrows solution
- Antibiotic therapy Keflex for 10 days
- Patient education
23
Therapeutic Interventions for impetigo
- Goal prevent scarring and promote self image.
- Individualize treatment to gender, age, and
severity of infection - Takes 4-6 wks to improve
- What is the major nursing implication here?
24
Candiditis- Thrush
- Overgrowth of Candida albicans
- Acquired through delivery
25
Thrush
- Characterized by white patches in the mouth,
gums, or tongue - Treated with oral Nystatin suspension swish
and swallow
26
Dermatophytosis (Ringworm)
- Tinea Capitis fungal
- infection known as
- ringworm
- Transmission
- Person-to-person
- Animal-to-person
27
SS
- Scaly, circumscribed patches to patchy, gray
scaling areas of alopecia. - Pruritic
- Generally asymptomatic, but severe, deep
inflammatory reaction may appear as boggy,
encrusted lesions (kerions)
28
- http//www.ecureme.com/quicksearch_reference.asp
29
Clinical manifestations
- Fungal infection of the stratum corneum, nails
and hair (the base of hair shaft causing hair to
break offrarely permanent) - Scaly, patches
- Pruritis
- Generally asymptomatic, but severe reactions may
appear as encrusted lesions
30
Tinea signs and symptoms
31
Therapeutic Interventions
- Transmitted by clothing, bedding, combs and
animals (cats especially) - May take 1-3 months to heal completely, even with
treatment - Child doesnt return to school until lesions dry
32
Diagnosis
- Potassium hydroxide examination
- Black Light
33
Medication Therapy
- Antifungals
- Oral griseofulvin (Lamisil)
- Give with fatty foods to aid in absorption
- Treatment is 4-6 wks
- Can return to daycare when lesions are dry
34
Pediculosis Capitis (lice)
-
http//www.emedicine.com/emerg/topic409.htm - a parasitic skin disorder caused by lice
- the lice lay eggs which look like white flecks,
attached firmly to base of the hair shaft,
causing intense pruritus
35
Diagnosis
- Direct identification of egg (nits)
- Direct identification of live insects
36
Pediculosis
37
Medication Therapy
- Treatment shampoos RID, NIX, Kwell(or Lindane)
shampoo is applied to wet hair to form a lather
and rubbed in for at least amount of time
recommended, followed by combing with a
fine-tooth comb to remove any remaining nits.
38
Scabies
- http//www.nlm.nih.gov/medlineplus/scabies.html
- Sarcoptes scabei mite. Females are 0.3 to 0.4 mm
long and 0.25 to 0.35 mm wide. Males are
slightly more than half that size. - A parasitic skin disorder (stratum corneum- not
living tissue) caused by a female mite. - The mite burrows into the skin depositing eggs
and fecal material between fingers, toes, palms,
axillae - pruritic grayish-brown, thread-like lesion
39
- http//www.aad.org/pamphlets_spanish/sarna.html
- Scabies between thumb and index finger
- On foot
40
Therapeutic Interventions
- transmitted by clothing, towels, close contact
- Diagnosis confirmed by demonstration from skin
scrapings. - treatment application of scabicide cream which
is left on for a specific number of hours (4 to
14)to kill mite - rash and itch will continue until stratum corneum
is replaced (2-3 weeks)
41
Care
- Fresh laundered linen and underclothing should be
used. - Contacts should be reduced until treatment is
completed.
42
(No Transcript)
Recommended
