
Primary Cytomegalovirus associated with interstitial pneumonitis and septic shock in an immunocompet - PowerPoint PPT Presentation
1 / 1
Title:
Primary Cytomegalovirus associated with interstitial pneumonitis and septic shock in an immunocompet
Description:
Primary Cytomegalovirus associated with interstitial pneumonitis and septic ... eMedicine from Web MD. 2005 Feb, 18. 3. Taylor G. Cytomegalovirus. Am Fam Physician. ... – PowerPoint PPT presentation
Number of Views:5018
Avg rating:3.0/5.0
Title: Primary Cytomegalovirus associated with interstitial pneumonitis and septic shock in an immunocompet
1
Primary Cytomegalovirus associated with
interstitial pneumonitis and septic shock in an
immunocompetent host
Kelly Fitzpatrick, MD1 Robert Holman, MD2
1Department of Medicine, Georgetown University
Hospital, Washington, DC 2Department of
Medicine, Virginia Hospital Center, Arlington, VA
Georgetown University
Abstract
Physical
Conclusions
Discussion
Vitals Temp 103.1 BP 114/59 P 116 RR
16 94 RA GEN Chills, AOx3, diffuse pink
lacy rash on back. HEENT Sclerae anicteric.
Conjuntiva mildly injected. PERRLA. EOMI. No LAD.
No TM. Neck supple. Dry MM. CV
Tachycardic. Normal S1,S2. No murmurs / rubs /
gallops. No JVD. PULM CTAB. ABD Soft,
NTND. NABS. No HSM. No CVA tenderness. EXT
No edema. 2 peripheral pulses bilaterally.
NEURO CN II-XII intact. 5/5 strength
throughout. Normal ROM. 2 DTR bilaterally.
Cytomegalovirus (CMV) belongs to the Herpes Virus
Family HHV-5.1,2,3 CMV consists of a
double-stranded DNA genome of more than 240 kbp,
capable of encoding more than 200 potential
protein products. Clinical specimens of CMV
contain cells with intranuclear inclusions, which
histopathologically have the appearance of owl's
eyes. The viral tegument, between the envelope
and the inner capsid, contains proteins that are
major targets of host cellmediated immune
responses. Host neutralizing antibody responses
and potential vaccines target glycoproteins on
the lipid bilayer. There are three classes of
viral replication.3 The first is immediate early
which involves transcription of an important
promoter gene. The remaining two classes, early
and late, involve transcription of DNA
replication and structural proteins, which are
the target of antiviral therapy. Treatment for
CMV includes viral DNA polymerase inhibitors such
as Ganciclovir 5mg/kg IV q 12, Foscarnet 90mg IV
q12. Cidofovir and Valganciclovir can also be
used. Other treatments include anti-CMV
benzimidazole ribosides, such as tomeglovir.
Clinical trials are currently investigating the
kinase inhibitor Maribavir and vaccines targeting
the lipid bilayer. CMV has various
manifestations including mononucleosis,
retinitis, pneumonitis, esophagitis,
gastroenteritis, hepatitis, pancreatitis,
colitis, cholecystitis, coagulopathy and
encephalitis.123 It is also included as one of
the congenital TORCH infections with potential
complications including sensorineural deafness,
microcephaly, psychomotor retardation,
hepatosplenomegaly, thrombocytopenia, rash and
blindness. CMV can be transmitted via saliva,
urine, cervicovaginal secretions, semen, fomites,
blood, organ transplant, breast milk and
placenta.
Primary Cytomegalovirus has been long recognized
as a cause of severe life-threatening infection
in immunocompromised hosts and now is also
emerging as a severe infection in immunocompetent
hosts. This clinical vignette describes a
healthy 35 year old male who presented with a
protracted febrile illness with vague flu-like
symptoms. Upon admission to the hospital the
patient was found to have a transamititis and the
patient developed severe pneumonitis progressing
to respiratory failure and requiring intubation.
Intravenous gangcyclovir was administered and the
patient recovered. Severe life-threatening cases
of CMV in immunocompetent hosts are seemingly
more common than previously thought and CMV may
not test seropositive early in presentation. CMV
should be in the differential for febrile
syndromes like that presented in this case report
so that appropriate antiviral therapy can be
administered as soon as possible.
Primary Cytomegalovirus has been long recognized
as a cause of severe life-threatening infection
in immunocompromised hosts and now is also
emerging as a severe infection in immunocompetent
hosts. Our case report presented a young healthy
adult with a febrile flu-like illness that
progressed to a life-threatening syndrome of
pneumonitis and hepatitis requiring intubation
and treatment in an intensive care unit.
Intravenous gangcyclovir was administered and the
patient recovered within one week. Severe
life-threatening cases of CMV in immunocompetent
hosts are seemingly more common than previously
thought and CMV may not test seropositive early
in presentation. CMV should be in the
differential for febrile syndromes like that
presented in this case report so that appropriate
antiviral therapy can be administered as soon as
possible.
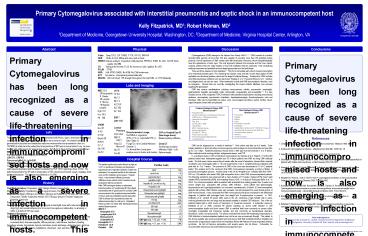
Labs and Imaging
WBC 12.6 38 Neutrophils 8 Bands 30
Lymphs 5 Monos 19 Atypical Lymphs Hgb
11.9 Hct 34.5 Plt 198 CHEM Na 137 K 4.0 Cl
102 Bicarb 28 BUN 9 Cr 1.1 Glu 106 Ca 8.2
- LFTS
- TP 5.9
- Alb 3.1
- Bili 1.3
- AST 181
- ALT 252
- AP 104
- ESR 7
- LDH 1946
- Lumbar Puncture
- Color clear
- WBC 3 RBC 1
- Polys 33, Monos 67
- Glu 78
- Prot 42
- Common Findings in Primary CMV Mononucleosis2,3
- Protracted fevers
- Absolute lymphocytosis with atypical lymphocytes
(50 monos, 10 atypical lymphs) - Heterophile Ab negative
- Rash (1/3)
- Cervical LAD (15)
- Transaminitis
- Mild to moderate anemia
- Reduced haptoglobin
- Elevated RF ANA ()
- Positive direct Coombs
- Polyclonal hypergammaglobulinemia
- Cryoglobulinemia
- Rare Findings in Primary CMV Mononucleosis2,3,4
- Pneumonitis
- Hepatitis
- Retitinis
- Colitis
- Pericarditis/ myocarditis
- Encephalitis
- Guillain-Barre Syndrome (CSF CMV DNA 1/3 cases
associated with development anti-GM2 Abs) - Thrombocytopenic purpura
- Vasculitis
- Thrombocytopenia
HPI
Bronchoalveolar Lavage No PMNS or organisms AFB
(-) Flu (-) Legionella DFA (-) EBV / CMV
(-) Fungal Cx rare Candida Albicans Giemsa
(-) Cx Normal flora, trace gram positive cocci
in chains and clusters
CXR on Hospital Day 3 (See image above)
Bilateral patchy infiltrates Chest CT Small
areas of patchy infiltrates. Right
Left Splenomegaly.
The patient is a 35 year old white male who
presented with fevers, rigors, shortness of
breath and cough for three weeks. The patients
symptoms were worse at night. He started having
generalized body aches and headaches early two
weeks earlier and presented in clinic on
10/19/06, at which time the patient had a
temperature of 99.5 and a normal chest X-ray. He
was treated with azithromycin for atypical
pneumonia, Tamiflu for 2 days and had several
labs drawn. WBC 4.3 Flu nasal swab (-) Monospot
(-) HIV AB (-) LDH 671 CRP 6.0 Parvovirus
IgM0.11 IgG3.60 CMV IgMIgGduring the day and went on a trip to Minnesota.
Persistent night sweats developed and the patient
contacted his PCP 10/31 reporting a fever of 102.
The patient presented to the ER with a
temperature of 103, shortness of breath, cough,
myalgias, back pain and headache. The patient
was admitted on 11/1/06.
References
- Cohen JI. Corey GR. Cytomegalovirus infection in
the normal host. Medicine 1985 64100. - 2. Schleiss M. Cytomegalovirus Infection.
eMedicine from Web MD. 2005 Feb, 18. - 3. Taylor G. Cytomegalovirus. Am Fam Physician.
2003 Feb 167(3)519-24. - 4. Steininger C. Popaw-Kraupp T. Seiser A . et
al. Presence of cytomegalovirus in cerebrospinal
fluid of patients with Guillain-Barre syndrome. J
Infect Disease 2004 189 984. - 5. Klemola E. Von Essen R. Henle G. Henle W.
Infectious-mononucleosis-like disease with
negative heterophil agglutination test. Clinical
features in relation to EBV and CMV antibodies.
J Infect Dis 1970 121608. - 6. Wreghitt TG. Teare EL. Sule O. Devi R. Rice P.
Cytomegalovirus Infection in Immunocompetent
Patients. Clinical Infectious Diseases 2003
3716031606. - 7. Rodríguez-Baño J. Muniain MA. Borobio MV.
Corral JL. Ramírez E. Perea EJ. Perez-Cano R.
Cytomegalovirus mononucleosis as a cause of
prolonged fever and prominent weight loss in
immunocompetent adults. Clinical Microbiology
Infection 2004 10 (5) 468-470. - 8. Eddleston M. Peacock S. Juniper M. Warrell DA.
Severe cytomegalovirus infection in
immunocompetent patients. Clin Infect Dis
19972452-6. - 9. Rafailidis PI. Mourtzoukou EG. Falagas ME.
Severe cytomegalovirus infection in apparently
immunocompetent patients a systematic review.
Virol J. 2008 Mar 27547.
CMV can be diagnosed by a variety of methods.2,3
Viral culture may take up to 6 weeks. Early
antigen detection or shell vial culture involves
exposing cell monolayers to monoclonal Abs and
may take up to 2 to 3 days. Radioimmunoassays
should show a CMV IgG four fold increase in 2 to
4 weeks. Other methods include serology
studies, antigenemia assays, and PCR. In a
landmark study in 1970 of infectious
mononucleosis by Klemola et al in Finland5, 72 of
the 494 patients tested were heterophile-negative
and 33 of these patients had CMV by rising CMV
antibody levels. The first serum, taken several
days to weeks after the onset of symptoms, showed
that a majority of patients were seronegative
(titer 14) and experienced a rise in
complement-fixing antibodies with peak titer at
4 to 7 weeks. The presence of CMV in the urine
was documented in 10 of 12 patients tested. This
analysis led to the conclusion that CMV
mononucleosis represents a primary infection in
previously seronegative persons. Another study
in the UK by Wreghitt et al.6 collected data from
1998 - 2001 on 124 patients who tested CMV IgM
seropositive from a total 7630 immunocompetent
patients. The following symptoms were observed
with a mean duration of 7.8 weeks malaise (67),
fever/ night sweats (46), transaminitis (69),
and relapsing illness (12). In a study by
Rodríguez-Baño et al.7 in 2004, four
immunocompetent adults presented with protracted
fever lasting greater than 6 weeks and severe
weight loss, associated with primary CMV
infection. Each patient had splenomegaly,
lymphocytosis and hypertriglyceridemia, but
recovered spontaneously. A further 20
immunocompetent patients with primary CMV
infection were also reviewed, and all presented
the usual clinical picture of CMV mononucleosis.
It was concluded that CMV mononucleosis should be
considered in the differential diagnosis in
patients with prolonged fever and weight loss if
lymphocytosis is present. In 1997, Eddleston et
al.8 studied 34 severe CMV cases in the UK,
observing a high mortality rate in cases
involving primarily the liver and lungs and
decreased mortality in isolated CSF infections.
Five of the six patients treated with a short
course of Ganciclovir or Foscarnet recovered. A
systematic review by Rafailidis et al.9 in 2008,
reviewed 89 articles reporting on severe CMV
infection in 290 immunocompetent adults and found
severe CMV to manifest itself more commonly as
severe colitis, meningitis, encephalitis and
transverse myelitis, and less commonly as
hematological disorders, thrombosis, uveitis, and
pneumonitis. The article concluded that severe
life-threatening complications of CMV infection
in immunocompetent patients may not be as rare as
previously thought. The patient in this clinical
vignette was immunocompetent and had severe CMV
that manifested itself as hepatitis and
pneumonitis progressing to septic shock and
respiratory failure with features of acute
respiratory distress syndrome. He did not become
seropositive until several weeks into his
illness. Fortunately, he recovered with
intravenous anti-viral treatment and supportive
care.
Hospital Course
The patient continued to spike fevers as high as
104.7 on levofloxacin therapy and developed
hypotension and respiratory distress 3 days into
admission. He required transfer to the intensive
care unit for intubation and pressors. Repeat
chest x-rays showed diffuse pulmonary
infiltrates verses edema most consistent acute
respiratory distress syndrome. After CMV
serologies drawn on admission became positive on
hospital day 3, the patient was treated with IV
gancyclovir for primary CMV mononucleosis. His
symptoms improved within 24 hours and was
extubated several days later. CMV viral load was
requested but was not obtained secondary to a lab
error. Outpatient follow-up CBC one week after
discharge showed marked lymphocytosis. WBC 8.1
Neutrophils 37.6 Lymphocytes 52.0
Monocytes 8.8 Eosinophils 0.8 Hemoglobin
12.1 Hematocrit 34.8 Platelets 284
Further Labs
History
Past Medical History Depression, ADD, Allergic
Rhinitis, Hemorrhoids. Past Social History
Tonsillectomy, Right inguinal hernia, Perianal
condyloma resection. Medications Allegra 180mg
po qd Lexapro 20mg po qd Adderall XL 15mg po
qd Azithromycin 5 day pack Tamiflu 4 capsules
Ambien CR 12.5mg po qhs prn Flonase Viagra prn
Propecia Xanax prn. Family History
Non-Contributory. Social History The patient is
adopted employed as hairstylist lives with male
partner and 2 dogs high risk sexual behavior
prior to current monogamous relationship no
smoking or IVDU 3-4 drinks ETOH per week. Review
of Symptoms Positives fever, night sweats,
cough, shortness of breath, myalgias, fatigue,
headache, impaired concentration and short term
memory, low back pain, mild right groin pain,
photosensitivity, increased thirst, decrease
appetite, diffuse joint pain, mild nausea,
heartburn, bloating. Negatives emesis,
hemoptesis, dysuria, hematuria, penile discharge,
abdominal pain, diarrhea, constipation, melena,
edema, palpitations, chest pain, rash, jaundice,
trauma.
Acknowledgments We would like to thank Dr. Joseph
Timpone and the Department of Medicine at
Georgetown University Hospital for their support
and encouragement.