
France : Par million dhabitants PowerPoint PPT Presentation
1 / 70
Title: France : Par million dhabitants
1
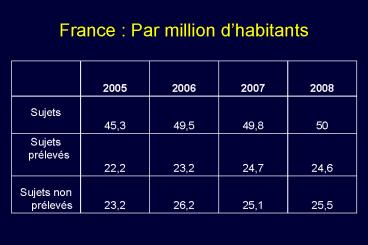
France Par million dhabitants
2
Causes de non prélèvement
3
Causes de la mort cérébrale
4
(No Transcript)
5
Non-heart beating donation (NHBD) The Maastricht
classification
6
Maastricht classification for Non-heart beating
donation (NHBD)
Categories I and II are termed uncontrolled and
categories III to V are controlled. Category II
donors are patients who have had a witnessed
cardiac arrest outside hospital, have
cardiopulmonary resusciation by trained
paramedics commenced within 10 minutes but who
cannot be successfully resuscitated. Category
III donors are patients on intensive care units
with non-survivable injuries who have treatment
withdrawn
7
Choix Europééns
- Niveau A interdiction Allemagne, Italie ?,
portugal, Hongrie - Niveau B Maastricht 1 et 2 seulement France,
Espagne - Niveau C Maastricht 3 seulement avec
gardes-fous éthiques UK, USA cote est - Niveau D Maastricht 3, accélération du
processus de mort, Maastricht 0 Pays-Bas - Niveau E Maastricht 3, accélération du
processus de mort, Maastricht 0 Belgique
8
France, dispositions légales et reglementaires
- DECRET
- Décret n 2005-949 du 2 août 2005 relatif aux
conditions de prélèvement des organes, des tissus
et des cellules et modifiant le livre II de la
première partie du code de la santé publique
(dispositions réglementaires) - Rapport de l'ABM sur l'application de la loi de
2004
9
(No Transcript)
10
(No Transcript)
11
Ethical Issues in Organ Donation After
Circulatory DeathGroupe Hospitalier
Pitié-SalpêtrièreNovember 24, 2008
- James L. Bernat, M.D.
- Professor of Neurology and Medicine
- Dartmouth Medical School
- Hanover, New Hampshire USA
12
DCD Definition
- Donation after circulatory death
- Scheduled organ procurement from a patient
declared dead by cessation of circulation and
respiration after life-sustaining treatment has
been withdrawn - Formerly called
- Non-heart-beating organ donation
- Organ donation after cardiac death
- Organ donation after cardio-circulatory death
13
DCD Process
- Ventilated patient in ICU with profound brain
damage who is not brain dead but cannot recover
neurologically - Family makes decision to withdraw LST based on
prognosis and wishes of patient - Family expresses desire to donate organs after
death with informed consent - Separate decisions to withdraw LST donate
14
DCD Process
- Organ donation coordinator counsels family and
makes arrangements to coordinate withdrawal of
life-sustaining treatment and organ procurement - Alert procurement team
- Schedule withdrawal of life-sustaining treatment
in ICU or OR - Bernat JL, et al. Am J Transplant
20066281-291.
15
DCD Process
- CCS staff extubates patient
- CCS staff provides usual palliative care with
opioids and benzodiazepines - Await apnea and asystole
- After 5 minutes of asystole, declare death
- Procure organs kidneys, liver, others
- 25 unsuccessful because no death lt 1 hour
- Bernat JL, et al. Am J
Transplant 20066281-291.
16
DCD History
- U. of Pittsburgh protocol, 1992
- National Academy of Sciences Institute of
Medicine reports in 1997, 2000, 2006 endorse DCD
and provide guidelines - In USA, encouraged by
- DHHS
- Joint Commission
- Steinbrook R. N Engl J Med
2007357209-213.
17
USA Deceased Organ Donors
9.8 of US deceased organ donors were DCD in 2007
18
New England Organ BankDeceased Organ Donors
25 of NEOB deceased organ donors were DCD in 2007
19
Kidneys comprised 74 of organs transplanted over
these four years
20
NEOB DCD Data
- Since 1 January 2004, 216 DCD donors of 328
attempted donations - 421 organs donated
- 346 kidneys
- 59 livers
- 9 pancreases
- Donor mean age 43.4 years
21
NEOB DCD Data
- Causes of death
- Anoxic brain injury 29
- Traumatic brain injury 35
- Stroke 29
- Other 11
22
DCD Ethical Issues
- Dead donor rule
- Circulatory-respiratory criterion of death
- Separation of withdrawal of LST from procurement
- Palliative care during dying
- Manipulation of living donor for organ
- ECMO on organ donor
- Procurement of hearts
- Bernat JL. N Engl J Med
2008359669-671.
23
Dead Donor Rule
- Multi-organ donor first must be dead
- It is unethical to kill the donor to procure
organs even with donor consent - Some have suggested abandonment of the dead donor
rule if - Patient consents for donation
- Patient is beyond harm
- Poor pubic policy because jeopardizes public
confidence in physicians
24
Circulatory Criterion of Death
- Irreversible cessation of circulation and
ventilation - Two definitions of irreversible
- Function cannot be reversed by present technology
(irreversible) - Function will not reverse itself because no
attempt will be made but possible (permanent) - Permanence is traditional standard
25
Irreversible vs Permanent in DCD
- At 5 minutes of asytole, respiratory and cardiac
functions are lost permanently - CPR will not be performed
- Auto-resuscitation will not occur
- Use of cardiopulmonary criterion in other
hospital deaths requires permanence and not
irreversibility - Bernat JL. J Clin Ethics
200617122-132.
26
Death Determination in DCD
- Permanence standard has been accepted implicitly
by the medical profession - Permanence always produces incipient, rapid, and
inevitable irreversibility - Its use is inconsequential in outcome
- Removing organs does not cause death
- Bernat JL. J Clin Ethics
200617122-132.
27
Circulatory Criterion of Death
- What duration of cessation of heartbeat shows
irreversibility? - Pittsburgh Protocol 2 minutes
- Institute of Medicine 5 minutes
- Empirical data on auto-resuscitation
- Organ damage from waiting longer
- SCCM Ethics Committee standard is not lt 2 minutes
or gt 5 minutes - Bernat JL, et al. Am J Transplant
20066281-291.
28
The Problem Inherent in DCD
- Is the patient truly dead after 5 minutes of
asystole? - If patient could be resuscitated to point of
measurable brain function, not dead - Supporters say its close enough to dead because
patient will not auto-resuscitate and no CPR is
planned - Bernat JL. J Clin Ethics
200617122-132.
29
Separation of Medical Roles
- Team declaring death must be totally separated
from team procuring organs - Particularly important in DCD where CCS team is
withdrawing LST - Decision to procure organs should not drive
decision to withdraw LST - USA case of Dr. Hootan Roozrokh problems of lack
of separation of roles - Bernat JL. N Engl J Med
2008359669-671.
30
Organ Donor Treatment
- Does palliative care of the donor contribute to
the time of death? - Is it ethical to manipulate the living organ
donor for the health of the organ? - IV phentolamine
- ECMO catheters
31
Emerging Unresolved Issues
- Variation among DCD protocols
- Minimum duration of asystole for death
declaration - Donor ECMO support
- Cardiac procurement
32
Organ Donor ECMO
- Extra-corporeal membrane oxygenation
- Donor ECMO catheters inserted while alive
- Deployed at moment death is declared
- Improves organ function by reducing warm ischemic
time - Retroactively negates donor death by preventing
progression to brain destruction - Jackson A, et al. J Heart Lung
Transplant 200827348-352.
33
DCD Organ Donor ECMO
- University of Michigan protocol insert thoracic
aorta occlusion balloon to block ECMO blood flow
to thoracic organs, brain - Permits progressive brain infarction as if ECMO
were not used - Acceptable because it avoids problem of
retroactive negation of donor death - Magliocca JF et al. J Trauma
2005581095-1102.
34
Heart Procurement in DCD
- HRSA-sponsored protocol successful heart
transplantation in 3 infants - Critics raised two questions
- Justified to reduce asystole period to 75 sec?
- Did use of donor heart negate the donors death
determination by showing that loss of cardiac
function was not irreversible ? - Boucek MM et al. N Engl J Med
2008359709-714.
35
Heart Procurement in DCD
- Death statute requires absence of circulatory not
cardiac function - Once circulation has ceased permanently, donor
patient is dead when brain is infarcted - Removal of heart and restarting it elsewhere has
no impact on donor status - Therefore, does not affect death determination
- Bernat JL. et al
(in press).
36
Future Directions
- Additional studies of auto-resuscitation
- Better standardization of DCD protocols
- Studies of physician DCD practice to identify
causality between stopping LST and DCD - Expert consensus on controversial areas ECMO,
cardiac procurement - HRSA committee meeting 15 December 2008
- Bernat JL. et
al (in press).
37
DCD Summary
- Definition, process, history
- Current status in USA
- Determination of death in DCD patient
- Ethical issues
- Unresolved issues
- ECMO donor support
- Heart procurement
- Future directions
38
CHWs Position on Donation After Cardiac Death
- Carol Bayley, Catholic Healthcare West
39
Old vs New
- Old DCD
- Death happened on its own terms
- Organs recovered but sometimes not in good
condition - New DCD
- Organs recovered in better condition
- Death is negotiated
40
Arguments in support of DCD
- Organ donation saves lives
- Pool of recipients has grown more quickly than
pool of donors - 90,000 on waiting list 6,000 die each yr
- DCD may honor pt/family wish
- Family may find comfort in donation
- Donation nurtures altruism
- DCD supported by transplant community
41
Arguments opposing DCD
- Conflict of interest
- DCD manipulates definition of death
- Pro literature first argued that Dead Donor Rule
not violated now same authors argue that
violation of DDR is justified. - Is it two, five or ten minutes?
- Permanent and irreversible depends on intentions
of those in OR
42
Arguments opposed, contd
- Do No Harm
- DCD procedures prior to taking organs may not be
in the patients best interest. (Ex) - Sometimes it doesnt work
- Patient is returned to floor to die
- Families may be disappointed
- Pressure to succeed strain on resources
43
Arguments Opposed, contd. Informed Consent
- Families are not told that testing procedures may
hasten death. - Families are not told that there is a ethical
debateOPOs do not believe there IS ethical
debate. - Substituted judgment difficult very few
individuals understand what is involved in
process. People with pink dot signed up for
something different.
44
Camels nose under the tent
- 15,00035,000 persons in PVS. Almost 2/3 of
medical directors and neurologists think PVS
patients appropriate for organ donation (1993) - Controlled suicidal donation
- High C-fracture, conscious patients
45
Delicate Consensus on End of Life Care may be
jeopardized
- Withdrawal of treatment is difficult
- Some resist because they think we are trying to
save money, or that the loved ones life is
worthless - DCD could backfire, resulting in fewer donations
overall
46
What is our duty?
- Hold to CHWs policy of no DCD transfer when
family requests. - Increase donations from brain dead patients
(e.g., St Johns) increase number of organs
recovered from each donor by following protocols
and calling OPO promptly.
47
Moral(s) of the Story
- Dying patients are not a means to anothers end,
even a good end. - Some things take time. Birth takes time death
takes time. - Patients are persons, not an assemblage of spare
parts.
48
Maastricht 0 ?
49
Belgian Transplantation Society20/03/08
- Organ Procurement after Euthanasia
- - Belgian Experience -
Ysebaert D, Van Beeumen G, Squifflet JP, Detry O,
De Roover A, Van Donink W, De Greef K, Roeyen G,
Chapelle T, Van Raemdonck D, Faymonville ME,
Laureys, S, Lamy M, Cras P, University Hospital
Antwerpen University Hospital Liège
50
(No Transcript)
51
Euthanasia
- Belgium Belgian Act on Euthanasia (May 28,
2002) - Euthanasia is described as an act on purpose,
performed by a third person, in order to end the
life of a person who has requested for this act.
- The patient is an adult or an emancipated minor,
capable and conscious at the time of his / her
request The request is made voluntarily, is well
thought out and reiterated, and is not the result
of outside pressure - The patient is in a hopeless medical condition
and complains of constant and unbearable physical
or mental pain which cannot be relieved
52
Euthanasia
- Belgium Belgian Act on Euthanasia
- If the person is not in the terminal phase of his
illness, the 2 doctors must consult with a third
doctor, either a psychiatrist or a specialist in
the disease concerned. - At least one month must pass between the written
request and carrying out the act - Every mercy killing must be reported to a federal
commission that would regulate the practice and
bring prosecutions where necessary.
53
Euthanasia in the World
- Once a Day in Belgium, Five a Day in Netherlands
- The Netherlands
- 2003, n1815 2004 n1886
- Belgium
- 2002 n170 14/month
- 2003 n235 19,6/month
- 2004 n349 29,1/month (87 Flanders)
- 2005 n393 32,7/month (84 Flanders)
54
Belgian experience patient data
55
(No Transcript)
56
Procedures
- Extensive written informed consent of donor and
relatives - Strict separation between euthanasie request -
euthanasia procedure organ procurement - Euthanasia performed by 2 physicians
neurologist - Euthanasia in wheelchair or bed, but in OR
- Organ retrieval after clinical diagnosis of
cardiac death by 3 physicians - Procedures performed by senior staff members and
nursing staff on a voluntary basis
57
Procedures
- Euthanasia procedure by overdose barbiturates,
muscle relaxation analgesia - Heparine given after euthanasia kit
- Organ procurement
- 3 x femoral vessel cannulation (DBTL catheter)
quick laparotomy for topical cooling (same
time) - 1 x quick laparotomy for topical cooling
- Organ allocation via Eurotransplant (allocation 4
hrs before) - Transplant centers informed about the nature of
the case and the elements of organ procurement
58
Belgian experience ischemia times
59
Belgian experience organ retrieval
All primary function !!!!!
60
Organ donation after euthanasia
- Potential ?
61
Conclusions
- Organ donation after euthanasia is feasable
- Strong patients wish to donate cannot be denied
- Clear separation between euthanasia request
euthanasia procedure organ procurement - High quality of NHBD-organs
- Potential of procedure
62
Category III donors Ethical issues
- The lack of organ through standard brain death
procedure increases the pressure on intensivists
to implement organ retrieval in patients for whom
a withdrawal of care decision has been taken - Apprehension of neurological outcome after major
brain injury through sophisticated MRI and EEG
techniques will undoubtfully improve within the
next years - The question of kidney and liver retrieval right
after cardiac arrest in major brain injured
patients according to the patients previous wish
or at the demand of the family might arise as our
skill to predict neurological outcome will
improve - This question is particularly relevant for our
practice since the best candidates regarding
organ viability are neurological patients
63
Category III donors Ethical issues
- However
- Category 3 patients have to progress swiftly from
withdrawal of care to asystole if organ function
is not to be compromised. - Death in the circumstances of major brain injury
is usually not rapid since other organ are well
functioning, the very reason why the entire
procedure is performed. - This is specially true at the second or third
week when MRI can be performed without any risk
to the patient - Death might have to be prompted through
increasing sedation in an extubated patient, or
by the administration of hypotensive agent, or
even NMB - This create ethical issues much more complicated
than those encountered in brain death
64
(No Transcript)
65
n43 severe TBI patients and 15
Controlsprincipal component analysis
66
Sn, Sp to predict poor outcomeBootstrap analysis
67
(No Transcript)
68
(No Transcript)
69
(No Transcript)
70
Conclusion HETEROGENEITE
- Explicable pour ce qui concerne les législations
sur le suicide médicalement assisté,
leuthanasie, les pratiques de LATA ? - Différences irréductibles en Europe ?
- Inexplicable au grand public pour le NHBD
- Maastricht 1 / 2 en France et en Espagne
- Maastricht 3 aux USA et en Belgique
- Maastricht 0 en Belgique
Recommended
