
STElevation Myocardial Infarction in the Oldest Old: PowerPoint PPT Presentation
1 / 1
Title: STElevation Myocardial Infarction in the Oldest Old:
1
ST-Elevation Myocardial Infarction in the Oldest
Old Clinical Outcomes and Quality of Life
Palak Shah, MD1, Amir H. Najafi MD2, Howard A.
Cooper MD FACC2
1Department of Medicine, Georgetown University
Hospital, Washington, 2Division of Cardiology,
Washington Hospital Center, Washington, DC
Equal contribution to this work
Georgetown University
Abstract
Results
However, limited data are available to guide
treatment in this age group, as the majority of
trials have specifically excluded the elderly.
Therefore, additional data regarding the
presentation, treatment, and short- and long-term
outcomes of STEMI are needed. In particular,
information regarding quality-of-life (QoL) among
STEMI survivors is of particular relevance to the
oldest old, but such data are currently lacking.
Based on these considerations, we evaluated the
short- and long-term outcomes including QoL
for consecutive patients aged 85 years treated
for STEMI in a single institution.
BACKGROUND The oldest old ( 85 years of age)
are the fastest growing segment of the US
population, but data are limited regarding the
treatment and outcomes of STEMI in this age
group. We sought to define the clinical course
of a large series of these patients admitted to a
single CCU. METHODS The presentation,
in-hospital treatment, and survival of
consecutive STEMI patients 85 years of age were
analyzed. Quality of life (QoL) was assessed
with the EQ-5D Index (range -0.11 to 1.00) and
EQ-VAS (range 0-100). RESULTS Of 1847 patients
admitted with STEMI from 2002-2007, 73 (4) were
85 years of age (range 85-94). Median time from
symptom onset to hospital arrival was 3 hours.
Cardiogenic shock occurred in 33. Primary PCI
was performed in 70 of patients, and procedural
success was 94. Evidenced-based therapy
included aspirin (97), clopidogrel (93), beta
blockers (82), ACE-I/ARBs (74), and statins
(86). In-hospital mortality was 32, and was
54 among those with cardiogenic shock.
Long-term follow up was obtained in 86 of
hospital survivors, among whom 1-year survival
was 82 and 2-year survival was 78. Cardiogenic
shock was the only independent predictor of
in-hospital mortality (OR 3.82, 95 CI
1.25-11.65, p0.02) and primary PCI was the only
independent predictor of long-term survival (HR
0.40, 95 CI 0.17-0.93, p0.02). Among survivors,
the mean EQ-5D Index was 0.780 0.038 and the
mean EQ-VAS was 70.45 4.46. CONCLUSION Among
the oldest old with STEMI, aggressive treatment
is associated with good long-term survival and
excellent QoL. The exception may be those
patients presenting with cardiogenic shock, in
whom short-term mortality remains exceedingly
high.
p lt 0.001
Methods
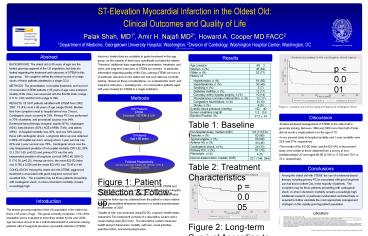
Figure 3 Long-term Survival According to
Presence of Cardiogenic Shock
1847 Patients STEMI Excluded NSTEMI U/A
Discussion
Table 1 Baseline Characteristics
- Evidenced-based management of STEMI in the oldest
old is generally lacking. Between 1996 and 2000
more than half of trials did not enroll a single
patient over the age of 75. - In our present study in-hospital mortality and
1-year mortality were 32 and 57, respectively. - The results of the EQ-5D index and the EQ-VAS in
the present study were similar to those obtained
from a survey of non-institutionalized US men
aged 80-89 (0.780 vs. 0.782 and 70.5 vs. 70.2,
respectively).
73 Patients Age 85 years
Followed Prospectively Clinical outcomes (Death,
MI, Stroke, CHF) Qol using EQ-5D
Table 2 Treatment Characteristics
Conclusions
Among the oldest old with STEMI, the use of
evidenced-based therapy including primary PCI is
associated with good long-term survival and
excellent QoL in the majority of patients. The
exception may be those patients presenting with
cardiogenic shock, in whom short-term mortality
remains exceedingly high. Additional research,
in particular randomized controlled trials, is
required to further elucidate the most
appropriate management strategies in this
rapidly-growing patient population.
Figure 1 Patient Selection Follow-up.
p 0.005
- Consecutive patients age 85 years presenting
with STEMI and admitted to the coronary care unit
(CCU) of the Washington Hospital Center between
October 2002 and September 2007 were included. - Long-term follow-up was obtained from the patient
or close relative utilizing standardized
telephone interviews or mailed questionnaires in
December of 2007. - Quality of Life was assessed using EQ-5D, a
generic health status instrument. The instrument
consists of a descriptive system and a visual
analog scale (EQ-VAS). The descriptive system
measures health along 5 dimensions mobility,
self care, usual activities, pain/discomfort, and
anxiety/depression.
Introduction
The fastest growing segment of the US population
is the oldest old, those 85 years of age. This
group currently comprises 1.3 of the population
and is expected to more than double by the year
2030. Age has been shown to be a critical
determinant of outcomes among patients with
ST-segment elevation myocardial infarction
(STEMI).
Literature
1. http//factfinder.census.gov, Accessed April
1, 2008. 2. Alexander KP, Newby LK, Armstrong PW,
et al. Acute coronary care in the elderly, part
II ST-segment-elevation myocardial infarction a
scientific statement for healthcare professionals
from the American Heart Association Council on
Clinical Cardiology in collaboration with the
Society of Geriatric Cardiology. Circulation
20071152570-89. 3. Lee PY, Alexander KP,
Hammill BG, Pasquali SK, Peterson ED.
Representation of elderly persons and women in
published randomized trials of acute coronary
syndromes. JAMA 2001286708-13. 4. Shaw JW,
Johnson JA, Coons SJ. US valuation of the EQ-5D
health states development and testing of the D1
valuation model. Med Care 200543203-20. 5. Mehta
RH, Rathore SS, Radford MJ, Wang Y, Krumholz HM.
Acute myocardial infarction in the elderly
differences by age. J Am Coll Cardiol
200138736-41. 6. Antman EM, Anbe DT, Armstrong
PW, et al. ACC/AHA guidelines for the management
of patients with ST-elevation myocardial
infarction a report of the American College of
Cardiology/American Heart Association Task Force
on Practice Guidelines (Committee to Revise the
1999 Guidelines for the Management of Patients
with Acute Myocardial Infarction). Circulation
2004110e82-292. 7. Hanmer J, Lawrence WF,
Anderson JP, Kaplan RM, Fryback DG. Report of
nationally representative values for the
noninstitutionalized US adult population for 7
health-related quality-of-life scores. Med Decis
Making 200626391-400.
Figure 2 Long-term Survival According to PCI
status
Recommended
