
Resurgence of Severe Group A Streptococcus Infections - PowerPoint PPT Presentation
1 / 1
Title:
Resurgence of Severe Group A Streptococcus Infections
Description:
CXR reveal right sided pneumonia (Picture 4) ... Developed ventilator associated pneumonia and penicillin was changed to meropenem ... – PowerPoint PPT presentation
Number of Views:77
Avg rating:1.0/5.0
Title: Resurgence of Severe Group A Streptococcus Infections
1
Resurgence of Severe Group A Streptococcus
Infections
Kathryn J. Sowerwine, MD Ram Srinivasan, MD
Princy N. Kumar, MD
Department of Medicine, Georgetown University
Hospital, Washington, DC Georgetown University
Medical Center, Washington, DC
Georgetown University
Case 2
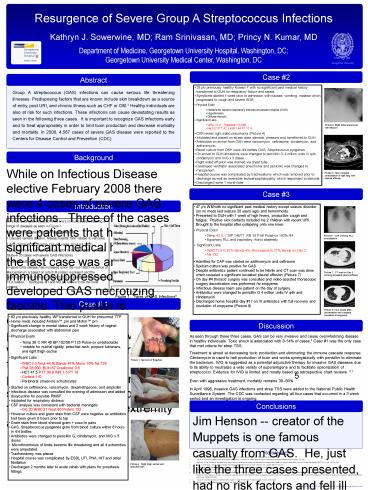
Abstract
- 29 y/o previously healthy Korean F with no
significant past medical history transferred to
GUH for respiratory failure and sepsis - Symptoms started 1 week prior to admission with
nausea, vomiting, malaise which progressed to
cough and severe SOB - Physical Exam
- Notable for severe respiratory distress at
outside hospital (OSH) - Hypotension
- Diffuse rhonchi
- Significant Labs
- WBC 12.2 Platelets 110,000
- Na 132 PTT 42.3 INR 1.44 PT 17.4
- CXR reveal right sided pneumonia (Picture 4)
- Intubated and placed on stress dose steroids,
pressors and transferred to GUH - Antibiotics on arrival from OSH were vancomycin,
ceftriaxone, clindamycin, and azithromycin. - Blood culture from OSH were 4/4 bottles GAS,
Streptococcus pyogenes - On arrival to GUH antibiotics were changed to
penicillin G 4 million units IV q4h, clindamycin
and IVIG x 3 doses - Right sided effusion was drained via chest tube
Group A streptococcus (GAS) infections can cause
serious life threatening illnesses. Predisposing
factors that are known include skin breakdown as
a source of entry, post URI, and chronic illness
such as CHF or DM.1 Healthy individuals are also
at risk for such infections. These infections can
cause devastating results as seen in the
following three cases. It is important to
recognize GAS infections early and to treat
appropriately in order to limit toxin production
and decrease morbidity and mortality. In 2006,
4,587 cases of severe GAS disease were reported
to the Centers for Disease Control and Prevention
(CDC).
Picture 4. Right sided pneumonia with effusion
C
Background
While on Infectious Disease elective February
2008 there were 4 cases of severe GAS infections.
Three of the cases were patients that had no
significant medical history and the last case was
an immunosuppressed patient that developed GAS
necrotizing fasciitis. This poster is dedicated
to the three previously healthy individuals with
GAS infections ranging from bacteremia with
pneumonia to full blown toxic shock meningitis
with purpura fulminans requiring 4 extremity
amputation.
Picture 5. Near complete consolidation of right
lung with minimal effusion
Case 3
Introduction
- 47 y/o WM with no significant past medical
history except seizure disorder (on no meds last
seizure 20 years ago) and hemorrhoids - Presented to GUH with 1 week of high fevers,
productive cough and fatigue. Positive sick
contacts included his 2 children with recent URI.
Brought to the hospital after collapsing onto
one knee. - Physical Exam
- Temp 40.6 C BP 146/77 RR 18 P 98 Pulse-ox 100
RA - Egophony RLL and inspiratory rhonci bilaterally
- Significant Labs
- WBC 12.6 N 87 Bands 4 ?increased to 27 Bands
on Day 2 - Na 132
- Admitted for CAP was started on azithromycin and
ceftrixone - Sputum culture was positive for GAS
- Despite antibiotics patient continued to be
febrile and CT scan was done which revealed a
significant loculated pleural effusion (Picture
7) - On day 4 thoracic surgery was consulted and
video-assisted thorascopic surgery decortication
was preformed for empyema - Infectious disease team saw patient on the day of
surgery - Antibiotics were changed to penicillin G 4
million units IV q4h and clindamycin.
- GAS has a complex interaction with ones immune
system causing a range of diseases as seen in
Figure 1. - Clusters of GAS infections have been observed
- Daycare centers (Boston, Massachusetts 1997
related to varicella) - Army barracks (Ft. Gordon, GA ?8 cases Jan-April
2007) - Long term living facilities (January 2001 to
October 2007 New York State? 35 cases with severe
GAS infections) - Hospital outbreaks
- Invasive GAS disease has increased since the
mid-1980s virulence of the bacterium is based on
which M protein is present and the host/humans
own immune reaction to the superantigen which may
be HLA related. 2 Serotypes M1 and M3 are known
to be the most virulent.3
Picture 6. CXR showing RLL consolidation
Picture 7. CT scan on Day 3 showing loculated
pleural effusion
Figure 1. Types of GAS Infections9
Case 1
Picture 8. Four weeks after presentation with
complete resolution of empyema
- 62 y/o previously healthy WF transferred to GUH
for presumed TTP - Home meds included Ambien prn and Motrin prn
- Significant change in mental status and 2 week
history of vaginal discharge associated with
abdominal pain - Physical Exam
- Temp 36C RR 40 BP 102/56 P 125 Pulse-ox
undetectable - notable for nuchal rigidity, petechial rash,
purpura fulminans, and right thigh eschar - Significant Labs
- WBC 2.3 Neut 44 Bands 41 Mono 10 Na 134
- Plat 28,000 BUN 67 Creatinine 3.6
- HCT 41.5 PTT 39.9 INR 1.3 PT 16
- Cortisol 110
- Peripheral smear-no schistocytes
- Started on ceftriaxone, vancomycin,
dexamethasone, and ampicillin - Infectious disease was consulted the evening of
admission and added doxycycline for possible RMSF
Discussion
.
As seen through these three cases, GAS can be
very invasive and cause overwhelming disease in
healthy individuals. Toxic shock is associated
with 8-14 of cases.5 Case 1 was the only case
that met criteria for strep TSS. Treatment is
aimed at decreasing toxic production and
eliminating the immune cascade response.
Clindamycin is used to halt production of toxin
and works synergistically with penicillin to
eliminate the bacterium. IVIG is suggested as a
potential adjunctive therapy for invasive GAS
diseases due to its ability to neutralize a wide
variety of superantigens and to facilitate
opsonization of streptococci. Evidence for IVIG
is limited and mostly based on retrospective
chart reviews. 6,7 Even with aggressive
treatment, mortality remains 3050.5 In April
1995, invasive GAS infections and strep TSS were
added to the National Public Health Surveillance
System. The CDC was contacted regarding all four
cases that occurred in a 3 week period and an
investigation is ongoing.
Picture 1. Necrosis of fingertips
Conclusions
Picture 2. Purpura fulminans
Jim Henson -- creator of the Muppets is one
famous casualty from GAS. He, just like the
three cases presented, had no risk factors and
fell ill to the toxic effects of GAS. There are
vaccines currently under investigation that would
potentially eliminate the spectrum of disease
from GAS.8 More research is needed to understand
why certain individuals are more susceptible than
others. Awareness of severe GAS infections will
help with early recognition and treatment.
References
- Demers, B. et al. Severe invasive group A
streptococcal infections in Ontario, Canada
1987-1991. Clin Infect Dis 16, 792-800 (1993). - Kotb, M. et al. An immunogenetic and molecular
basis for differences in outcomes of invasive
group A streptococcal infections. Nat Med
Published online November 18, 2002. - Vlaminckx, B. et al. Site-specific manifestations
of invasive group a streptococcal disease type
distribution and corresponding patterns of
virulence determinants. Journal of Clinical
Microbiology, 2003 (Vol. 41) (No. 11) 4941-4949 - Baxter, F, McChesney, J Severe group A
streptococcal infection and streptococcal toxic
shock syndrome. Can J Anesth 200047,1129-1140 - S. Mehta et al. Stewart Morbidity and Mortality
of Patients With Invasive Group A Streptococcal
Infections Admitted to the ICUChest,December1, 20
06 130(6) 1679 1686 - Norrby-Teglund, A and Stevens, DL. Novel
therapies in streptococcal toxic shock syndrome
attenuation of virulence factor expression and
modulation of the host response. Curr Opin Infect
Dis 199811,285-291ISI - Basma, H, Norrby-Teglund, A, McGeer, A, et al
Opsonic antibodies to the surface M protein of
group A streptococci in pooled normal
immunoglobulins (IVIG) potential impact on the
clinical efficacy of IVIG therapy for severe
invasive group A streptococcal infections. Infect
Immun 199866,2279-2283 - Journal Of The American Medical Association
(2004, August 11). Early Results Show Promise For
Strep Vaccine. ScienceDaily. - http//www.nfsuk.org.uk/Information/strepa2.php
The 'Lee Spark' NF Foundation.
Picture 3. Right thigh eschar and petechial rash