
A%20Randomized%20Trial%20of%20Rosuvastatin%20in%20the%20Prevention - PowerPoint PPT Presentation
Title: A%20Randomized%20Trial%20of%20Rosuvastatin%20in%20the%20Prevention
1
(No Transcript)
2
(No Transcript)
3
(No Transcript)
4
JUPITER Trial Presented during AHA 2008
Scientific Sessions
A Randomized Trial of Rosuvastatin in the
Prevention of Cardiovascular Events Among 17,802
Apparently Healthy Men and Women With Elevated
Levels of C-Reactive Protein (hsCRP) The
JUPITER Trial Paul Ridker, Eleanor Danielson,
Francisco Fonseca, Jacques Genest, Antonio Gotto,
John Kastelein, Wolfgang Koenig, Peter
Libby, Alberto Lorenzatti, Jean MacFadyen, Borge
Nordestgaard, James Shepherd, James Willerson,
and Robert Glynn on behalf of the JUPITER Trial
Study Group
5
Independent Steering Committee P Ridker
(Chair), F Fonseca, J Genest, A Gotto, J
Kastelein, W Koenig, P Libby, A Lorenzatti, B
Nordestgaard, J Shepherd, J Willerson Independent
Academic Clinical Coordinating Center P
Ridker, E Danielson, R Glynn, J MacFadyen, S Mora
(Boston) Independent Academic Study
Statistician R Glynn (Boston) Independent Data
Monitoring Board R Collins (Chair), K Bailey, B
Gersh, G Lamas, S Smith, D Vaughan Independent
Academic Clinical Endpoint Committee K Mahaffey
(Chair), P Brown,D Montgomery, M Wilson, F Wood
(Durham)
6
JUPITER
- JUPITER is the first large-scale, prospective
study to examine the role of statin therapy in
individuals with low to normal LDL-C levels, but
with increased cardiovascular risk identified by
elevated CRP - It assessed the long-term impact of rosuvastatin
in individuals potentially at increased
cardiovascular risk due to elevated CRP levels
who do not qualify for lipid-lowering treatment
according to current guidelines
Adapted from Ridker et al. N Eng J Med 2008359
2195-207.
7
JUPITER - Rationale
- Nearly half of all cardiovascular events occur in
patients who are apparently healthy and who have
low or normal levels of LDL-C - hsCRP predicts cardiovascular disease independent
of LDL-C levels - Along with improved screening there is a need to
examine the use of lipid-lowering agents as a
method of reducing the risk of cardiovascular
events
Adapted from Ridker PM. Circulation 2003 108
2292-97. Ridker PM. Am J Cardiol 2007 100
1659-64. Ridker PM. New Engl J Med 2002 347
1557-65. Ridker PM. Am J Cardiol
200392(suppl)17K-22K.
8
JUPITER Background and Prior Work
Current guidelines for the prevention of
myocardial infarction stroke, and cardiovascular
death endorse statin therapy among patients with
established vascular disease, diabetes, and
among those with hyperlidemia. However, these
screening and treatment strategies are
insufficient as half of all heart attack and
stroke events occur among apparently healthy men
and women with average or even low levels of
cholesterol.
Adapted from Ridker et al .NEJM 2008.
9
JUPITER Background and Prior Work
To improve detection of individuals at increased
risk for cardiovascular disease, physicians often
measure high sensitivity C-reactive protein
(hsCRP), an inflammatory biomarker that
reproducibly and independently predicts future
vascular events and improves global risk
classification, even when cholesterol levels are
low. Prior work has shown that statin therapy
reduces hsCRP, and that among stable coronary
disease patients as well as those with acute
ischemia, the benefit associated with statin
therapy relates not only to achieving low levels
of LDL, but also to achieving low levels of
hsCRP.
Adapted from Ridker et al. NEJM 2008.
10
Efficacy of lovastatin in AFCAPS/TexCAPS
subgroups by baseline LDL-C and hsCRP
Study group Rate of cardiovascular events Rate of cardiovascular events NNT
Lovastatin Placebo NNT
Low LDL-C/low hsCRP 0.025 0.022 N/A
Low LDL-C/high hsCRP 0.029 0.051 48
High LDL-C/low hsCRP 0.020 0.050 33
High LDL-C/high hsCRP 0.038 0.055 58
Median LDL-C3.9 mmol/L (149 mg/dL). Median
hsCRP1.6 mg/L AFCAPS/TexCAPSAir Force/Texas
Coronary Atherosclerosis Prevention Study
hsCRPhigh-sensitivity C-reactive protein
LDL-Clow-density lipoprotein cholesterol
N/Anot applicable NNTnumber needed to treat to
prevent one coronary event
Adapted from Ridker et al. N Engl J Med
20013441959-65.
11
JUPITER population compared with previous trials
in patients without established CHD
AFCAPS WOSCOPS JUPITER
Patients, n 6605 6595 17 802
male 85 100 62
Duration, years 5.2 4.9 1.9
Diabetes, 6 1 0
Baseline lipids, mmol/L
total cholesterol 5.72 7.03 4.73
LDL-C 3.88 4.97 2.69
HDL-C 0.931.03 1.14 1.32
triglycerides 1.78 1.85 1.56
hsCRP, mg/L 0.2 NA 4.3
Statin Lovastatin 2040 mg Pravastatin 40 mg Rosuvastatin 20 mg
CVDcardiovascular disease CHDcoronary heart
disease LDL-Clow-density lipoprotein
cholesterol HDL-Chigh-density lipoprotein
cholesterol hsCRPhigh sensitivity C-reactive
protein AFCAPSAirforce/Texas Coronary
Atherosclerosis Prevention Study WOSCOPSWest of
Scotland Coronary Prevention Study Baseline
lipid levels are mean values.
Adapted from Ridker et al. Am J Cardiol
20071001659-64. Ridker et al. N Engl J Med.
20013441959-65.
12
Comparison of the JUPITER Trial Population to
Previous Statin Trials of Primary Prevention
JUPITER WOSCOPS
AFCAPS Sample size (n) 17,802 6,595
6,605 Women (n) 6,801
0 997 Minority (n) 5,118
0 350 Duration (yrs) 1.9 (max 5)
4.9 5.2 Diabetes ()
0 1 6 Baseline LDL-C
(mg/dL) 108 192
150 Baseline HDL-C (mg/dL) 49
44 36-40 Baseline TG (mg/dL)
118 164
158 Baseline hsCRP (mg/L) gt 2
NA NA Intervention Rosuvastatin Prav
astatin Lovastatin 20 mg 40 mg 10-40
mg
Adapted from JUPITER Trial Study Group, Am J
Cardiol 2007.
13
JUPITER Why Consider Statins for Low LDL, high
hsCRP Patients?
In 2001, in an hypothesis generating analysis of
apparently healthy individuals in the AFCAPS /
TexCAPS trial, we observed that those with low
levels of both LDL and hsCRP had extremely low
vascular event rates and that statin therapy did
not reduce events in this subgroup (N1,448, HR
1.1, 95 CI 0.56-2.08). Thus, a trial of statin
therapy in patients with low cholesterol and low
hsCRP would not only be infeasible in terms of
power and sample size, but would be highly
unlikely to show clinical benefit. In contrast,
we also observed within AFCAPS/TexCAPS that among
those with low LDL but high hsCRP, vascular event
rates were just as high as rates among those with
overt hyperlipidemia, and that statin therapy
significantly reduced events in this subgroup
(N1,428, HR 0.6, 95 CI 0.34-0.98).
Adapted from Ridker et al. N Engl J Med
20013441959-65.
14
JUPITER Why Consider Statins for Low LDL, High
hsCRP Patients?
AFCAPS/TexCAPS Low LDL Subgroups
Low LDL, Low hsCRP Low LDL, High hsCRP
Low LDL, Low hsCRP Low LDL, High hsCRP
A
B
2.0
0.5
1.0
2.0
0.5
1.0
RR
Statin Effective
Statin Not Effective
Statin Effective
Statin Not Effective
However, while intriguing and of potential public
health importance, the observation in
AFCAPS/TexCAPS that statin therapy might be
effective among those with elevated hsCRP but low
cholesterol was made on a post hoc basis. Thus,
a large-scale randomized trial of statin therapy
was needed to directly test this hypotheses.
Adapted from Ridker et al. New Engl J Med
20013441959-65.
15
JUPITER - Objective
- The primary objective was to investigate whether
long-term treatment with rosuvastatin 20 mg
decreases the rate of first major cardiovascular
events compared with placebo in patients with low
to normal LDL-C but at increased cardiovascular
risk as identified by elevated CRP levels.
Adapted from Ridker et al. Circulation
20031082292-97.
16
JUPITER Trial Design
JUPITERMulti-National Randomized Double Blind
Placebo Controlled Trial of Rosuvastatin in the
Prevention of Cardiovascular EventsAmong
Individuals With Low LDL and Elevated hsCRP
MI Stroke Unstable Angina CVD Death CABG/PTCA
Rosuvastatin 20 mg (N8901)
No Prior CVD or DM Men gt50, Women gt60 LDL lt130
mg/dL hsCRP gt2 mg/L
Placebo (N8901)
4-week run-in
Argentina, Belgium, Brazil, Bulgaria, Canada,
Chile, Colombia, Costa Rica, Denmark, El
Salvador, Estonia, Germany, Israel, Mexico,
Netherlands, Norway, Panama, Poland, Romania,
Russia, South Africa, Switzerland, United
Kingdom, Uruguay, United States, Venezuela
Adapted from Ridker et al. Circulation
20031082292-97.
17
JUPITER Study Design
No history of CAD men 50 yrs women 60
yrs LDL-C lt130 mg/dL CRP 2.0 mg/L
Rosuvastatin 20 mg (n8901)
Placebo run-in
Placebo (n8901)
16
24
30
413
VisitWeek
Final
6-monthly
Lead-in/eligibility
Lipids CRP Tolerability
Lipids CRP Tolerability HbA1C
Randomisation
Lipids CRP Tolerability
Median follow-up 1.9 years
CADcoronary artery disease LDL-Clow-density
lipoprotein cholesterol CRPC-reactive protein
HbA1cglycated haemoglobin
Adapted from Ridker et al. N Eng J Med
20083592195-207.
18
JUPITER 17,802 Patients, 1,315 Sites, 26
Countries
25
4021
20
Total Randomized 17,802
2873
15
2497
2020
Randomizations ( Total.)
10
987
804
5
741
487
345
336
327
273
270
253
222
209
204
202
197
162
143
85
83
32
15
14
0
Chile
Canada
Uruguay
Estonia
Israel
Panama
Russia
Mexico
Poland
Romania
El Salvador
Bulgaria
Norway
Belgium
Germany
Costa Rica
Brazil
Denmark
Colombia
Venezuela
Argentina
South Africa
Switzerland
United States
United Kingdom
The Netherlands
Adapted from Ridker et al. NEJM 2008.
19
JUPITER - Patient Flow
89,890 subjects screened 17,802 randomised
Rosuvastatin 20mg n8,901
Placebo n8,901
Lost to follow up n44
Lost to follow up n37
Completed study n8,857
Completed study n8,864
Adapted from Ridker et al. N Eng J Med 2008359
2195-207.
20
JUPITER Inclusion and Exclusion Criteria, Study
Flow
89,890 Screened
89,863 Screened
Reason for Exclusion () LDL gt 130 mg/dL
52 hsCRP lt 2.0 mg/L
36 Withdrew Consent 5 Diabetes
1 Hypothyroid
lt1 Liver Disease lt1 TG gt 500
mg/dL lt1 Age out of range
lt1 Current Use of HRT lt1 Cancer
lt1 Poor
Compliance/Other 3
Reason for Exclusion () LDL-C gt 130 mg/dL
53 hsCRP lt 2.0 mg/L 37 Withdrew
Consent 4 Diabetes
1 Hypothyroid lt1 Liver
Disease lt1 TG gt 500 mg/dL
lt1 Age out of range
lt1 Current Use of HRT lt1 Cancer
lt1 Poor Compliance/Other
3
Men gt 50 years Women gt 60 years No CVD, No DM LDL
lt 130 mg/dL hsCRP gt 2 mg/L
4 week Placebo Run-In
17,802 Randomized
17,802 Randomized
8,901 Assigned to Rosuvastatin 20 mg
8,901 Assigned to Placebo
8,901 Assigned to Placebo
8,901 Assigned to Rosuvastatin 20 mg
8,600 Completed Study 120 Lost to follow-up
8,857 Completed Study 44 Lost to follow-up
8,864 Completed Study 37 Lost to follow-up
8,600 Completed Study 120 Lost to follow-up
8,901 Included in Efficacy and Safety Analyses
8,901 Included in Efficacy and Safety Analyses
8,901 Included in Efficacy and Safety Analyses
8,901 Included in Efficacy and Safety Analyses
Adapted from Ridker et al. NEJM 2008.
21
JUPITER - Major Exclusion Criteria
- Current use of statins or other lipid-lowering
therapies - Current use of post menopausal hormone
replacement therapy - Prior history of cardiovascular or
cerebrovaascular events, such as MI, unstable
angina, prior arterial revascularisation or
stroke, or CHD-risk equivalents - Chronic inflammatory condition, such as severe
arthritis, lupus or inflammatory bowel disease
and/or treatment with immunosuppressants - Uncontrolled
- hypertension SBP gt 190 mmHg or DBP gt 100 mmHg
- hypothyroidism TSH gt 1.5 x ULN
- CK ?3 x ULN
- Serum creatinine gt 2.0 mg/dL
- Evidence of hepatic dysfunction (ALT gt 2 x ULN)
- History of prior malignancy, alcohol or drug abuse
CHD coronary heart disease CK creatinine
kinase ULN upper limit of normal SBP
systolic blood pressure DBP diastolic blood
pressure
Adapted from Ridker et al. N Eng J Med
20083592195-207. Ridker PM. Circulation
20031082292-97.
22
JUPITER - Baseline Characteristics
Rosuvastatin Placebo n8901 n8901
Age (years) 66 (60-71) 66 (60-71) Male sex ()
61.5 62.1 Race () White 71.4 71.1 Black 12.4
12.6 Hispanic 12.6 12.8 Other 3.6 3.5 BMI
(kg/m2) 28.3 (25.3-32.0) 28.4 (25.3-32.0) Systoli
c BP (mmHg) 134 (124-145) 134 (124-145) Diastoli
c BP (mmHg) 80 (75-87) 80 (75-87)
All values are median (interquartile range) or N
().
Adapted from Ridker et al. N Eng J Med
20083592195-207.
23
JUPITER Baseline Blood Levels (median,
interquartile range)
Rosuvastatin Placebo (N
8901) (n 8901) hsCRP, mg/L 4.2 (2.8 -
7.1) 4.3 (2.8 - 7.2) LDL, mg/dL 108 (94
- 119) 108 (94 - 119) HDL, mg/dL 49 (40
60) 49 (40 60) Triglycerides, mg/L 118 (85 -
169) 118 (86 - 169) Total Cholesterol,
mg/dL 186 (168 - 200) 185 (169 - 199) Glucose,
mg/dL 94 (87 102) 94 (88 102) HbA1c,
5.7 (5.4 5.9) 5.7 (5.5 5.9) All
values are median (interquartile range).
Mean LDL 104 mg/dL
Adapted from Ridker et al. NEJM 2008.
24
JUPITER - Baseline laboratory parameters
Rosuvastatin Placebo na8901
n8901
Total cholesterol (mmol/L) 4.81 (4.34-5.17) 4.78
(4.37-5.15) LDL cholesterol (mmol/L) 2.79
(2.43-3.08) 2.79 (2.43-3.08) HDL cholesterol
(mmol/L) 1.27 (1.03-1.55) 1.27
(1.03-1.55) Triglycerides (mmol/L) a1.33
(0.96-1.91) 1.33 (0.97-1.91) hsCRP (mg/L) 4.2
(2.8-7.1) 4.3 (2.8-7.2) Glucose (mmol/L) 5.2
(4.8-5.7) 5.2 (4.9-5.7) HbA1c() 5.7
(5.4-5.9) 5.7 (5.5-5.9) Glomerular filtration
rate, (ml/min/1.73m2) 73.3 (64.6-83.7) 73.6
(64.6-84.1)
For hsCRP, values are the average of the values
obtained at two screening visits
All values are median (interquartile range) or N
().
Adapted from Ridker et al. N Eng J Med 2008359
2195-207.
25
JUPITER - Medical History
Medical History Rosuvastatin
Placebo n8901
n8901
Current smoker () 15.7 16.0 Family history
CHD () 11.2 11.8 Metabolic syndrome
() 41.0 41.8 Aspirin use () 16.6 16.6
Family history of premature coronary heart
disease (CHD) defined as first degree relative
with CHD at age lt 55 yrs (male), lt 65 yrs
(female) Metabolic syndrome defined according
to consensus criteria of American Heart
Association and the National Heart, Lung, and
Blood Institute
Adapted from Ridker et al. N Eng J Med 2008359
2195-207.
26
JUPITER - Study End Points
- Primary End Point
- Time to the first occurrence of a major
cardiovascular event, composite of - cardiovascular death
- Stroke
- MI
- unstable angina
- arterial revascularisation
- Secondary End Points
- total mortality
- non-cardiovascular mortality
- development of diabetes mellitus
- development of venous thromboembolic events
- bone fractures
- discontinuation of study medication due to
adverse effects.
Adapted from Ridker et al. Circulation
20031082292-97.
27
JUPITER Primary Objectives
Justification for the Use of statins in
Prevention an Intervention Trial Evaluating
Rosuvastatin
To investigate whether rosuvastatin 20 mg
compared to placebo would decrease the rate of
first major cardiovascular events among
apparently healthy men and women with LDL lt 130
mg/dL (3.36 mmol/L) who are nonetheless at
increased vascular risk on the basis of an
enhanced inflammatory response, as determined by
hsCRP gt 2 mg/L. To enroll large numbers of
women and individuals of Black or Hispanic
ethnicity, groups for whom little data on primary
prevention with statin therapy exists.
Adapted from Ridker et al. NEJM 2008.
28
JUPITER Effects of Rosuvastatin 20 mg on LDL,
HDL, TG, and hsCRP
LDL (mg/dL)
HDL (mg/dL)
LDL decrease 50 percent at 12 months
HDL increase 4 percent at 12 months
hsCRP (mg/L)
TG (mg/dL)
hsCRP decrease 37 percent at 12 months
TG decrease 17 percent at 12 months
0
12
24
36
48
Months
Months
Adapted from Ridker et al. NEJM 2008.
29
JUPITER Adverse Events and Measured Safety
Parameters
Event Rosuvastatin Placebo P Any
SAE 1,352 (15.2) 1,337 (15.5) 0.60 Muscle
weakness 1,421 (16.0) 1,375 (15.4) 0.34 Myopath
y 10 (0.1) 9 (0.1) 0.82 Rhabdomyol
ysis 1 (0.01) 0 (0.0) -- Incident
Cancer 298 (3.4) 314 (3.5) 0.51 Cancer
Deaths 35 (0.4) 58 (0.7) 0.02 Hemor
rhagic stroke 6 (0.1)
9 (0.1) 0.44 GFR (ml/min/1.73m2 at 12 mth)
66.8 (59.1-76.5) 66.6 (58.8-76.2) 0.02 ALT gt
3xULN 23 (0.3) 17 (0.2) 0.34 Fastin
g glucose (24 mth) 98 (91-107)
98 (90-106) 0.12 HbA1c ( at 24 mth) 5.9
(5.7-6.1) 5.8 (5.6-6.1) 0.01 Glucosuria (12
mth) 36 (0.5) 32 (0.4) 0.64 Incident
Diabetes 270 (3.0) 216 (2.4) 0.01
Occurred after trial completion, trauma induced.
All values are median (interquartile range)
or N () Physician reported
Adapted from Ridker et al. NEJM 2008.
30
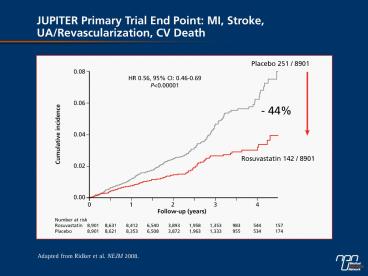
JUPITER Grouped Components of the Primary End
Point
Myocardial Infarction, Stroke, or Cardiovascular
Death
Arterial Revascularization or Hospitalization for
Unstable Angina
HR 0.53, CI 0.40-0.70 Plt0.00001
HR 0.53, CI 0.40-0.69 Plt0.00001
0.05
0.06
Placebo
Placebo
0.05
0.04
0.04
- 47
0.03
Cumulative Incidence
Cumulative Incidence
- 47
0.03
0.02
0.02
Rosuvastatin
Rosuvastatin
0.01
0.01
0.00
0.00
0
1
2
3
4
0
1
2
3
4
Follow-up (years)
Follow-up (years)
Adapted from Ridker et al. NEJM 2008.
31
JUPITER Individual Components of the Primary
End Point
Endpoint Rosuvastatin Placebo HR 95CI
P Primary Endpoint 142 251 0.56
0.46-0.69 lt0.00001 Non-fatal MI 22 62 0.35
0.22-0.58 lt0.00001 Any MI 31 68 0.46
0.30-0.70 lt0.0002 Non-fatal Stroke 30 58 0.5
2 0.33-0.80 0.003 Any Stroke 33 64 0.52
0.34-0.79 0.002 Revascularization or
Unstable Angina 76 143 0.53 0.40-0.70 lt0.00001
MI, Stroke, CV Death 83 157 0.53
0.40-0.69 lt0.00001
Nonfatal MI, nonfatal stroke,
revascularization, unstable angina, CV death
Adapted from Ridker et al. NEJM 2008.
32
JUPITER Primary End Point Subgroup Analysis I
N
P for Interaction
Men
11,001
0.80
Women
6,801
Age
lt
65
8,541
0.32
Age gt 65
9,261
Smoker
2,820
0.63
Non-Smoker
14,975
Caucasian
12,683
0.57
Non-Caucasian
5,117
USA/Canada
6,041
0.51
Rest of World
11,761
Hypertension
10,208
0.53
No Hypertension
7,586
All Participants
17,802
0.25
0.5
1.0
2.0
4.0
Rosuvastatin Superior
Rosuvastatin Inferior
Adapted from Ridker et al. NEJM 2008.
33
JUPITER - Primary End PointTime to first
occurrence of a CV death, non-fatal stroke,
non-fatalMI, unstable angina or arterial
revascularisation
Hazard Ratio 0.56 (95 CI 0.46-0.69) Plt0.00001
Placebo
0.08
0.06
Cumulative Incidence
Rosuvastatin 20 mg
0.04
NNT for 2 yrs 95 5 yrs 25
0.02
0.00
0
1
2
3
4
5
Years
Number at risk Rosuvastatin 8901 8412
3893 1353
538 157 Placebo 8901 8353
3872 1333
531 174
Extrapolated figure based on Altman and Andersen
method
Adapted from Ridker et al. N Eng J Med
20083592195-207.
34
JUPITER Primary Endpoint Subgroup Analysis II
N
P for Interaction
Family HX of CHD
2,045
0.07
No Family HX of CHD
15,684
2
4,073
0.70
BMI lt 25 kg/m
7,009
BMI 25-29.9 kg/m
2
6,675
BMI
gt
30 kg/m
2
Metabolic Syndrome
7,375
0.14
No Metabolic Syndrome
10,296
Framingham Risk
lt
10
8,882
0.99
Framingham Risk gt 10
8,895
hsCRP gt 2 mg/L Only
6,375
hsCRP gt 2 mg/L Only
6,375
All Participants
17,802
0.25
0.5
1.0
2.0
4.0
Rosuvastatin Superior
Rosuvastatin Inferior
Adapted from Ridker et al. NEJM 2008.
35
JUPITER Secondary End Point All Cause Mortality
Adapted from Ridker et al. NEJM 2008.
36
JUPITER Statins and the Development of Diabetes
HR (95 CI)
WOSCOPS Pravastatin
0.70 (0.500.98)
1.34 (1.061.68)
PROSPER Pravastatin
1.20 (0.981.35)
HPS Simvastatin
1.20 (0.911.44)
ASCOT-LLA Atorvastatin
PROVE-IT Atorvastatin VS Pravastatin
1.11 (0.671.83)
JUPITER Rosuvastatin
1.25 (1.051.54)
Statin Better
Statin Worse
Adapted from Ridker et al. NEJM 2008.
37
JUPITER Predicted Benefit Based on LDL
Reduction vs Observed Benefit
Proportional reduction in vascular event rate
(95 CI)
CTT
JUPITER PREDICTED
TNT
PROVE-IT
A-to-Z
IDEAL
Mean LDL cholesterol differencebetween treatment
groups (mmol/L)
Adapted from Ridker et al. NEJM 2008.
38
JUPITER Predicted Benefit Based on LDL
Reduction vs Observed Benefit
Proportional reduction in vascular event rate
(95 CI)
Mean LDL cholesterol differencebetween treatment
groups (mmol/L)
Adapted from Ridker et al. NEJM 2008.
39
Prevalence of conventional risk factors in male
patients with CHD
Four (0.9)
Three
None
8.9
19.4
Two
27.8
43.0
One
Total male patients87 869CHDcoronary heart
disease smoking, hypertension,
hypercholesterolaemia and diabetes mellitus
Adapted from Khot et al. JAMA 2003290898-904.
40
CRP is a strong independent predictorof CV
events in women
Lp(a) Homocysteine IL-6 TC LDL-C sICAM-1 SAA
ApoB TC/HDL-C CRP CRP TC/HDL-C
0
1.0
2.0
4.0
6.0
Relative risk of future CV events
Apoapolipoprotein CRPC-reactive protein
CVcardiovascular HDL-Chigh-density lipoprotein
cholesterol ILinterleukin LDL-Clow-density
lipoprotein cholesterol Lp(a)lipoprotein (a)
SAAserum amyloid A sICAM-1soluble
intercellular adhesion molecule 1 TCtotal
cholesterol
Adapted from Blake GJ, Ridker PM. Circ Res
200189763-71.
41
CRP predicts risk of MI and strokein apparently
healthy men
2.0
3.5
3.0
1.5
2.5
Relativerisk of ischaemicstroke
Relative risk of MI
2.0
1.0
1.5
1.0
0.5
0.5
0
0
1
2
3
4
1
2
3
4
Quartile of CRP
Quartile of CRP
CRPC-reactive protein MImyocardial
infarctionQuartile 1 0.55 Quartile 2
0.56-1.14 Quartile 3 1.15-2.10 Quartile 4 ?
2.11. P0.02 versus quartile 1 Plt0.001
versus quartile 1
Adapted from Ridker et al. N Engl J Med
1997336973-79.
42
CV event-free survival in women using combined
LDL-C and hsCRP measures
1.00
Low LDL-C, low hsCRP
0.99
Probability of event-free survival
High LDL-C, low hsCRP
0.98
Low LDL-C, high hsCRP
0.97
High LDL-C, high hsCRP
0.96
0
CVcardiovascular hsCRPhigh-sensitivity
C-reactive protein LDL-Clow-density lipoprotein
cholesterol Median LDL-C3.2 mmol/L (124
mg/dL) Median CRP1.5 mg/L
Adapted from Ridker et al. N Engl J Med
20023471557-65.
43
JUPITER Subgroup Analysis
Placebo better
Rosuvastatin better
0.2
0.4
0.6
0.8
1.2
0
N P- value
Age 0.32
65 years 8,541
gt65 yrs 9,261
Gender 0.80
Males 11,001
Females 6,801
Race 0.57
White 12,683
Non-white 5,117
Hypertension 0.53
Yes 10,208
No 7,586
Region 0.51
US or Canada 6,041
Other 11,761
Metabolic syndrome Metabolic syndrome 0.14
Yes 7,375
No 10,296
Family history of CHD Family history of CHD 0.07
Yes 2,045
No 15,684
Framingham risk score Framingham risk score 0.99
10 8,882
gt10 8,895
1
Hazard ratio (95 CI)
Adapted from Ridker et al. N Eng J Med 2008359
2195-207.
Recommended
CrystalGraphics Presentations



























