
Enormous Economic Consequences of Diabetes in the United States - PowerPoint PPT Presentation
1 / 44
Title:
Enormous Economic Consequences of Diabetes in the United States
Description:
1 tube glucose gel. 1/3 to cup of fruit juice. 1 cup skim milk. 1/3 to cup of regular soda. 6 small sugar cubes. 1 tbsp honey. 5 lifesavers ... – PowerPoint PPT presentation
Number of Views:98
Avg rating:3.0/5.0
Title: Enormous Economic Consequences of Diabetes in the United States
1
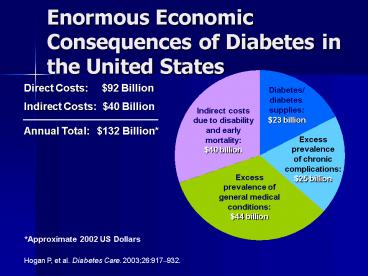
Enormous Economic Consequences of Diabetes in the
United States
Direct Costs 92 Billion
Diabetes/ diabetes supplies 23 billion
Indirect Costs 40 Billion Annual Total
132 Billion
Indirect costs due to disability and early
mortality 40 billion
Excess prevalence of chronic complications 25
billion
Excess prevalence of general medical
conditions 44 billion
Approximate 2002 US Dollars
Hogan P, et al. Diabetes Care. 200326917932.
2
Impact of Type 1 and Type 2 Diabetes
6th leading cause of death
Individuals diagnosed? by 1.3 million each year
Increasingly affects all age groups
Diabetes
Shortens average life expectancy by up to 15
years
Especially prevalent in African and Hispanic
Americans
Adapted from http//www.cdc.gov/diabetes/pubs/fact
sheet.htmcontents. Accessed 2/10/04. Diabetes
Research Working Group. NIH Pub
99-439819991129.
3
Type 2 Accounts for the Vast Majority of Diabetes
Mellitus Cases
- Type 2 diabetes
- About 75 of the diabetes population
- Dual impairment Insulin deficiency Insulin
resistance - No longer a disease of adults only
- Obesity
- Genetic link
- Type 1 diabetes
- Approximately 10 of diabetes population
- Absolute insulin requirement
- Autoimmune mediated
CDC. National Diabetes Fact Sheet. 2003 Atlanta,
GA. US Dept. HHS, Center for Disease Control and
Prevention 2003.
4
Prediabetes
- Historically has been called impaired glucose
tolerance, or borderline diabetes - Very high probability of leading to diabetes
- Broadly defined as a fasting glucose of
110-125mg/dl or impaired glucose tolerance of
140-199 mg/dl 2 hours after a 75 gram glucose
load
5
Metabolic syndrome(syndrome X)
- This syndrome is a relatively recently recognized
group of characteristics that puts a patient at
risk for type 2 diabetes. They include - Central obesity
- Hypertension
- Hyperlipidemia
- Insulin resistance or glucose intolerance
- Proinflammatory state
6
Prevalence of Diabetes Is Escalating
2001
(Includes Gestational Diabetes)
Source Mokdad A, et al. Diabetes Care.
2000231278-1283 Mokdad A, et al. J Am Med
Assoc. 200128610 Mokdad A, et al. JAMA.
200328976-79.
7
The Role of the Pancreas in Blood Sugar Regulation
- Alpha Cells
- Glucagon
- Acts on liver to release glycogen
- Increases blood sugar
- Delta Cells
- Somatostatin
- Stops glucagon and growth hormone
- Decreases blood sugar
- Beta Cells
- Insulin
- Decreases blood sugar
Colorado State University. http//arbl.cvmbs.colo
state.edu/hbooks/pathphys/endocrine/pancreas/anato
my.html. Accessed December 3, 2003.
8
Normal Physiologic Insulin Sensitivity and
?Cell Function Produce Euglycemia
Normal Insulin Sensitivity
Normal ?Cell Function
Decreased Lipolysis
Pancreas
Liver
Decreased Plasma FFA
? Glucose Uptake
? Glucose Production
Islet ?Cell DegranulationInsulin Released in
Response to Elevated Plasma Glucose
Muscle
Adipose Tissue
Decreased Glucose Output
Normal Physiologic Plasma Insulin
Increased Glucose Transport
Euglycemia
9
Type 1 Diabetes
Inflammation
FasL
IFNg
TNFa
- Beta cell destruction
- Usually leading to absolute insulin deficiency
- Immune mediated
- Idiopathic
T cell
Autoimmune Reaction
Macrophage
TNFa
Class IMHC
Class IIMHC
IL-1
Beta cell
NO
CD8 T cell
Dendritic cell
Beta cell Destruction
American Diabetes Association. Diabetes Care.
200326S33S50.
10
Progression of Type 1 Diabetes
Precipitating event
Progressive loss of insulin release
Genetic predisposition
Antibody formation
Normal insulin release
Glucose normal
Beta Cell Mass
Overt diabetes
C-peptide present
No C-peptide present
Time
Atkinson MA and Eisenbarth GS. Lancet.
2001358221229.
11
Beta Cell Dysfunction and Insulin Resistance
Produce Hyperglycemia in Type 2 Diabetes
Insulin Resistance
Beta Cell Dysfunction
Increased Lipolysis
Pancreas
Liver
Elevated Plasma FFA
?Glucose Uptake
?Glucose Production
Islet Beta Cell DegranulationReduced Insulin
Content
Muscle
Adipose Tissue
Increased Glucose Output
Reduced Plasma Insulin
Decreased Glucose Transport and Activity
(expression) of GLUT4
Hyperglycemia
Setter S, et al. In Herfindal T, Gourley D, eds.
Textbook of TherapeuticsDrug and Disease
Management. 7th ed. 2000377406.
12
Prevalence of Diabetes
- Magnitude of the Disease
13
AgeAdjusted Total Prevalence of Diabetes in
People Aged 20 Years or Older, by
Race/EthnicityUnited States, 2002
American Indians/Alaskan Natives
Hispanic/Latino Americans
Non-Hispanic African Americans
Non-Hispanic Caucasians
0
10
20
25
15
5
Percent
Source 1999-2001 National Health Interview
Survey and 1999-2000 National Health and
Nutrition Examination Survey estimates projected
to year 2002. 2002 outpatient database of the
Indian Health Service.
14
(No Transcript)
15
Prevalence of Diabetes at Age 45 to 74 Years
16
How and why diabetes affects major physiologic
systems
- Objective 3
17
Metabolic Complication Pathways
- Advanced Glycosylation Endproducts
- Sorbitol (polyol) Pathway
18
Advanced Glycosylation Endproducts (AGEs)
- Circulation glucose attaches to various proteins
via a process called glycosylation - Glucose attaches to the amino terminus of the
protein forming aldimine (Schiff base) which
later irreversibly changes through an amadori
reaction to AGEs
19
AGEs
- AGEs are found in both extracellular and
intracellular sites. - These AGEs then form irreversible
protein-protein crosslinks with other amino
groups, that permanently attach to macromolecules
such as arterial wall collagen
20
AGEs sites affected
- Other sites affected by AGEs are macrophages,
endothelial cells, and smooth muscle. - AGEs accumulate over the life of the patient.
- AGEs in arterial walls can increase binding for
LDL cholesterol
21
AGEs sites affected
- AGE formation also causes the thickening of
capillary basement membranes. - This process is thought to be responsible for the
microvascular complications in the eye, kidney,
and nerve cells
22
Sorbitol pathway
- Some cells are not dependent on insulin for entry
of glucose (brain and eye) - Glucose enters these cells and is enzymaticaly
converted to sorbitol and fructose
23
Sorbitol pathway-complications
- Elevated glucose levels within the cell leads to
an increase in formation of sorbitol and
fructose. These two sugars accumulate within the
cell and create a hyperosmolar state. This
increases the amount of water being pulled within
the cell which leads to swelling and cell damage.
24
Sorbitol pathway - complications
- The cellular damage as a result of this process
is what leads to damage of the fine blood vessels
in the retina and peripheral nervous system.
25
Complications of Diabetes
Cardiovascular complications
Renal failure
Blindness
Diabetes
Amputation
Nerve damage
http//www.cdc.gov/diabetes/pubs/factsheet.htmcon
tents. Accessed 2/10/04.
26
Chronic Complications
- Complications due to chronic hyperglycemia are
microvascular, macrovascular, and neuropathic - Microangiopathy damage to smaller arteries by
diffuse thickening of the capillary basement
membranes - Macroangiopathy damage to larger blood vessels
27
Physiologic systems affected
- Vascular system
- The three major types of macrovascular disease
complications in diabetes are CAD (responsible
for 50-60 of deaths), cerebrovascular disease,
and peripheral vascular disease (PVD). - Accelerated atherosclerosis in the major arteries
increase risk of MI, cerebral stroke, aortic
aneurysms, and gangrene of lower extremities
28
Physiologic systems
- Diabetic nephropathy (microangiopathy)
- Found in 20 - 30 or patients with diabetes
- Renal failure accounts for many deaths in both
type 1 and type 2 patients - Symptom include microalbuminuria, proteinuria,
chronic renal failure, and HTN - ACE inhibitors help prevent this damage in
addition to tight glucose control
29
Physiologic systems
- Ocular complications (microvascular)
- Proliferative and nonproliferative retinopathy,
cataracts and glaucoma - Damage due to weakened blood vessels
- Osmotic damage can also occur to the lens of the
eye and certain neurons, by the sorbitol pathway
metabolism of glucose. - Risk factors poor blood glucose control, high
blood pressure, hyperlipidemia
30
Physiologic systems
- Neuropathy (neurologic/microvascular)
- Classified as somatic and autonomic
- Affect 50 of patients
- May affect nearly every system of the body
- Occurs due to accumulation of sorbitol, and
decrease in myoinositol, nerve glyosylation, - Somatic
- The most common.
- Lead to decreased sense of touch, position, and
vibration sensations. Painful sensations also
occur such as tingling, pin pricks
(parasthesias), burning, stabbing, tearing, even
crushing pain - Sweat glands also affected. Decreased
moisture/dry skin
31
Neuropathy cont.
- Autonomic
- Affects the involuntary nerves of the autonomic
nervous system - Complications occur include gastroparesis,
diarrhea, constipation, urinary tract
dysfunction, sexual dysfunction, and cardiac
abnormalities.
32
Physiologic systems
- Infections
- Decreased ability to fight infections
- Prolonged healing times
- Due to impaired leukocyte function and poor
circulation - Infections in the mouth can lead to gum disease
33
Frequent Symptoms of Diabetes
- May be asymptomatic at in type 2
- 3 Ps
- polyuria,
- polydipsia,
- Polyphagia
- Ketoacidosis
- Weakness/fatigue
- Glycosuria
- Dry, itchy skin
- Visual changes
- Skin and mucous membrane infections
34
Normal Plasma glucose range
- Normal fasting plasma glucose is 70-110
mg/dl - Diagnostic criteria for diabetes
- Fasting plasma glucose of 126mg/dl or a 2 hour
postload glucose of 200mg/dl. Must be
confirmed on a different day. - Diagnostic criteria for pre-diabetes
- Fasting plasma glucose of 100-125mg/dl or a 2
hour postload glucose of 140-199 mg/dl
35
Importance of Postprandial Glucose (PPG)
Conclusions
- Even in nondiabetic individuals, postprandial
hyperglycemia carries a higher risk of death than
elevated fasting evidence shows that elevated PPG
levels increases the risk for cardiovascular
disease - Earlier detection and management of postprandial
hyperglycemia is crucial in reducing the risk of
death
Gerich J. Arch Int Med. Jun 20031631306-1316
36
Conclusions
- Approximately 13 million patients in the United
States have diabetes, with another 5.2 million
people undiagnosed - US health care costs associated with diabetes are
132 billion each year - Kidney failure, cardiovascular disease,
blindness, and amputations are major
complications of diabetes - Intensive insulin therapy is effective in
reducing the risk of several diabetic
complications - Use of intensive insulin therapy is steadily
increasing
37
Risk factors associated with development of Type
2 diabetes
- Family history
- Children of individuals with type 2 diabetes have
a 15 chance of developing the disease and 30
risk of developing IGT - 90 concordance in twins
- Obesity 120 of ideal body weight
- Age 45yo
- Race
- History of gestational diabetes
- Hypertension
- Hyperlipidemia
- Polycystic ovary disease
38
HbA1c
- Hemoglobin is a protein in circulating red blood
cells. The level of glycosylation to HbA1c of
this protein is directly proportional to the
level of glucose in the blood. Because
gylcosylation is irreversible and the life span
of a red blood cell is 120 days, measuring the
level can tell us how well blood sugar has been
controlled over the past 3 to 4 months. - Should be
39
Approximate Comparison of HbA1c to Blood Glucose
- Glucose mg/dl
HbA1c
40
Blood glucose test vs. urine glucose test
- Blood glucose testing tells you what your blood
sugar is at that time. The kidney only spills
glucose into the urine when blood glucose levels
exceed 180mg/dl. So urine testing is not very
accurate and the results only approximate what
your blood sugar level was at an earlier time.
41
Hyperglycemia
- High blood sugar. 200 mg/dl
- Symptoms include
- Extreme thirst
- Frequent urination
- Dry skin
- Hunger
- Blurred vision
- Drowsiness
- Nausea
- If not corrected can lead to diabetic
ketoacidosis
42
Hypoglycemia
- Low blood sugar
- Symptoms include
- Shaky, light-headed or weak
- Sweaty or clammy skin
- Fast heartbeat
- Irritability
- Confusion
- Sudden extreme hunger
- Headache
- Fast heartbeat
43
Treatment of hypoglycemia
- Rule of 15s
- If blood sugar is low eat or drink 15 grams of
carbohydrate - Wait 15 minutes
- Check blood sugar again
- If blood glucose is normal and your next meal is
more than 60 to 90 minutes away eat a snack - If not back to normal then treat, wait and check
again. If not back to normal after 3 tmts. Call
911
44
Hypoglycemia
- 15 grams of carbohydrate
- 4 glucose tablets
- 1 tube glucose gel
- 1/3 to ½ cup of fruit juice
- 1 cup skim milk
- 1/3 to ½ cup of regular soda
- 6 small sugar cubes
- 1 tbsp honey
- 5 lifesavers
Recommended
CrystalGraphics Presentations























![NOTE: To appreciate this presentation [and ensure that it is not a mess], you need Microsoft fonts: PowerPoint PPT Presentation](https://s3.amazonaws.com/images.powershow.com/5528768.th0.jpg?_=202007270510)
![NOTE: To appreciate this presentation [and ensure that it is not a mess], you need Microsoft fonts: PowerPoint PPT Presentation](https://s3.amazonaws.com/images.powershow.com/5816511.th0.jpg?_=20200718068)
![NOTE:%20To%20appreciate%20this%20presentation%20[and%20ensure%20that%20it%20is%20not%20a%20mess],%20you%20need%20Microsoft%20fonts:%20%20 PowerPoint PPT Presentation](https://s3.amazonaws.com/images.powershow.com/P1247176264UDuye.th0.jpg?_=201805141011)


![NOTE: To appreciate this presentation [and insure that it is not a mess], you need Microsoft fonts: PowerPoint PPT Presentation](https://s3.amazonaws.com/images.powershow.com/7010443.th0.jpg?_=20150809053)
![NOTE:%20To%20appreciate%20this%20presentation%20[and%20insure%20that%20it%20is%20not%20a%20mess],%20you%20need%20Microsoft%20fonts:%20%20 PowerPoint PPT Presentation](https://s3.amazonaws.com/images.powershow.com/P1252428420wZXYW.th0.jpg?_=20180601048)