
WATER METABOLISM - PowerPoint PPT Presentation
1 / 36
Title:
WATER METABOLISM
Description:
Acute intermittent porphyria. Shy-Drager syndrome. Head injury. Lung disease. Pneumonia ... Acute psychosis. Post-operative state. AIDS. Glucocorticoid ... – PowerPoint PPT presentation
Number of Views:354
Avg rating:3.0/5.0
Title: WATER METABOLISM
1
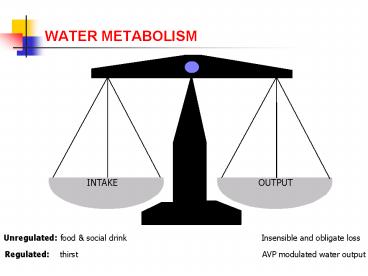
WATER METABOLISM
Unregulated food social drink Insensible
and obligate loss
Regulated thirst AVP modulated water
output
2
THIRST
- Hyperosmolar stimulus
- hypothalamic osmoreceptors
- threshold 1 to 4 above basal
- Hypovolaemic stimulus
- baroreceptors
- threshold 10 - 15
- ? absent in man (inconvenient with postural
change!) - Normally inactive as unregulated input is in
excess
3
BASAL
4
AVP secretion
- Synthesized in hypothalamic SON and PVN nuclei
- Stored and released from posterior pituitary (gt 1
week store!) - Interacts via V2 receptors to insert aquaporin-2
water channels - Osmolar threshold within normal range
- High gain (i.e steep curve and high renal
sensitivity)
5
(No Transcript)
6
AVP secretion
- Osmotic stimulus high sensitivity
- Hypovolaemic stimulus high threshold (gt10)
7
(No Transcript)
8
AVP secretion
- Osmotic stimulus high sensitivity
- Hypovolaemic stimulus high threshold (gt10)
- Nausea most powerful known
- Stress e.g. post-operative
- Drugs SIADH
9
INTEGRATION OF THIRST AND AVP
- Unregulated water intake supplies water in excess
of need - Excess water is excreted
- AVP secretion regulates free water clearance
- AVP maintains osmolality within narrow limits
- This avoids inconvenient thirst and
water-seeking behaviour - Thirst kicks-in when deficiency reaches harmful
levels
10
DIFFERENTIAL DIAGNOSIS OF HYPONATRAEMIA
HYPONATRAEMIA
Pseudo- hyponatraemia
YES
Lipaemia / hyperproteinaemia ?
NO
Compensatory hyponatraemia
Hyperglycaemia ?
YES
NO
Volume expanded
Volume depleted
Total body water
Renal loss
Extra-renal loss
No oedema
Oedema
Diuretics Addisons
Vomiting Diarrhoea
SIADH Hypothyroid
Nephrotic Cirrhosis CCF
UNa
gt20
lt10
lt10
gt20
Rx
Normal saline
Fluid restriction
11
Causes of hyponatraemia
HYPONATRAEMIA
Pseudo- hyponatraemia
YES
Lipaemia / hyperproteinaemia ?
NO
Compensatory hyponatraemia
Hyperglycaemia ?
YES
NO
Volume expanded
Volume depleted
Total body water
Renal loss
Extra-renal loss
No oedema
Oedema
Diuretics Addisons
Vomiting Diarrhoea
SIADH Hypothyroid
Nephrotic Cirrhosis CCF
UNa
gt20
lt10
lt10
gt20
Rx
Normal saline
Fluid restriction
12
Causes of hyponatraemia
HYPONATRAEMIA
Pseudo- hyponatraemia
YES
Lipaemia / hyperproteinaemia ?
NO
Compensatory hyponatraemia
Hyperglycaemia ?
YES
NO
Volume expanded
Volume depleted
Total body water
Renal loss
Extra-renal loss
No oedema
Oedema
Diuretics Addisons
Vomiting Diarrhoea
SIADH Hypothyroid
Nephrotic Cirrhosis CCF
UNa
gt20
lt10
lt10
gt20
Rx
Normal saline
Fluid restriction
13
Case 1
- A 58-year old man presented with a history of
general malaise and a persistant painful cough of
three months duration - Serum
- Sodium 116 mmol/L
- Potassium 3.4 mmol/L
- Urea 9.4 mmol/L
- Bilirubin 12 umol/L
- Alk phos 95 U/L
- ALT 23 U/L
- Albumin 20 g/L
- Total protein 120 g/L
14
Causes of hyponatraemia
HYPONATRAEMIA
Pseudo- hyponatraemia
YES
Lipaemia / hyperproteinaemia ?
NO
Compensatory hyponatraemia
Hyperglycaemia ?
YES
NO
Volume expanded
Volume depleted
Total body water
Renal loss
Extra-renal loss
No oedema
Oedema
Diuretics Addisons
Vomiting Diarrhoea
SIADH Hypothyroid
Nephrotic Cirrhosis CCF
UNa
gt20
lt10
lt10
gt20
Rx
Normal saline
Fluid restriction
15
(No Transcript)
16
Case 3
- A 66-year old man was admitted for investigation
of possible bronchogenic carcinoma - Serum Ref range
- Sodium 121 mmol/L 133 143
- Potassium 4.1 mmol/L 3.6 4.6
- Urea 4.4 mmol/L 3.0 7.0
17
Case 3
- A 66-year old man was admitted for investigation
of possible bronchogenic carcinoma - Serum Ref range
- Sodium 121 mmol/L 133 143
- Potassium 4.1 mmol/L 3.6 4.6
- Urea 4.4 mmol/L 3.0 7.0
- Glucose 5.2 mmol/L
18
Case 3
- A 66-year old man was admitted for investigation
of possible bronchogenic carcinoma - Serum Ref range
- Sodium 121 mmol/L 133 143
- Potassium 4.1 mmol/L 3.6 4.6
- Urea 4.4 mmol/L 3.0 7.0
- Glucose 5.2 mmol/L
- Osmolality 250 mmol/Kg 275 - 295
- Urine
- Osmolality 614 mmol/Kg
19
SYNDROME OF INAPPROPRIATE ADH
- Hyponatraemia is very common
- up to15 hospitalised patients
- affects 50 of nursing home residents each year
- gt30 acutely ill nursing home patients have
hyponatramia - SIADH accounts for about 50 of all chronic
hyponatraemias
20
SYNDROME OF INAPPROPRIATE ADH
- Bartter and Schwartz criteria (1967)
- hyponatraemia with hypotonicity of plasma
- urine osmolality inappropriately high
- ongoing renal sodium excretion
- absence of oedema or volume depletion
- normal renal and adrenal function
- i.e. normovolaemic hyponatraemia
21
SYNDROME OF INAPPROPRIATE ADH
Symptoms relate to rate of fall as well as
severity
- Sodium lt120 mmol/L
- Lethargy
- Anorexia
- Nausea and vomiting
- Irritability
- Headache
- Muscle weaknes
- Cramps
- Sodium lt110 mmol/L
- Drowsiness
- Confusion
- Depressed reflexes
- Extensor plantar responses
- Seizures
- Coma
- Death
No oedema because water distributed in both
compartments
22
SIADH - pathogenesis
- Inappropriately high AVP levels
- Ongoing (unregulated) water intake
- Blood volume rises
- gt10 expansion inhibits aldosterone and triggers
natriuresis
23
Causes of SIADH
- Neoplasia
- Carcinoma of lung, pancreas, bladder
- Leukaemia
- Thymoma
- Lymphoma
- Sarcoma
- Mesothelioma
- Neurological disorders
- Meningitis
- Encephalitis
- Brain tumour
- Subarachnoid haemorrhage
- Cerebral and cerebellar atrophy
- Guillain-Barré syndrome
- Acute intermittent porphyria
- Shy-Drager syndrome
- Head injury
- Lung disease
- Pneumonia
- TB
- Pneumothorax
- Asthma
- IPPV
24
Causes of SIADH
- Drugs
- Vasopressin
- Oxytocin
- Vinca alkaloids
- Cisplatin
- Chlorpropamide
- Carbamazepine
- Phenothiazines
- Thiazides
- MAOIs
- SSRIs
- Tricyclics
- Nicotine
- Ecstacy
- Miscellaneous
- Acute psychosis
- Post-operative state
- AIDS
- Glucocorticoid deficiency
- Severe hypothyroidism
- Idiopathic
25
The impact of ageing on water metabolism
- Rise in osmotic sensitivity of ADH release
- Delayed ability to excrete water load
- Thirst mechanism diminishes
- Decrease in maximal urinary concentrating ability
- Decreased renal mass
- Impaired responsiveness to sodium balance
- Multiple drug therapy
- A lifetime of accumulated disease and
comorbidities
26
The impact of ageing on water metabolism
- Rise in osmotic sensitivity of ADH release
- Delayed ability to excrete water load
- Thirst mechanism diminishes
- Decrease in maximal urinary concentrating ability
- Decreased renal mass
- Impaired responsiveness to sodium balance
- Multiple drug therapy
- A lifetime of accumulated disease and
comorbidities
27
Patterns of AVP release in SIADH
28
Diagnosis of SIADH
- Essential criteria
- True plasma hypo-osmolality (lt275 mOsm/Kg)
- Inappropriate urine osmolality (gt100 mOsm/Kg)
- Euvolaemia no oedema, ascites or intravascular
hypovolaemia - Urine sodium not low (gt30 mmol/L during normal
intake) - Normal renal, adrenal, and thyroid function
- Supplemental criteria
- Low serum urea and urate
- Unable to excrete gt80 of water load (20mL/Kg) in
4h and/or failure to achieve urine osmolality
lt100 mOsm/Kg - No significant rise in serum Na after volume
expansion but improvement with fluid restriction
29
Treatment of SIADH
- Identification and treatment of underlying cause
- Clearance of excess water
- not necessary in asymptomatic chronic
hyponatraemia - fluid restriction to 500 - 1000 mL/24h
- Demeclocycline
- 600 to 1,200 mg daily
- may take three weeks to reach maximal effect
- caution in renal or hepatic insufficiency
- Specific V2 receptor antagonists (OPC-31260)
30
Treatment of SIADH
- Hypertonic saline
- Only if significantly symptomatic or duration lt3
day - Calculate sodium required
- Na req. (mmol) (125 Na) x 0.6 x body
weight (kg) - Also measure and re-infuse urinary sodium output
- Rate of increase not usually gt0.5 mmol/L/h
- ? combine with i.v. furosemide
- Stop saline when sodium reaches 120 - 125 mmol/L
31
Treatment of SIADH
Na req. (mmol) (125 Na) x 0.6 x body
weight (kg)
- Example symptomatic patient with sodium 105
mmol/L - Body weight 60 Kg
- Available hypertonic saline 2.7 (3 normal)
- Sodium requirement (125-105) x 0.6 x 60 720
mmol - 2.7 saline Na 462 mmol/L
- Correction at 0.5 mmol/L/hr ? correction over 25
hrs - 2.7 saline requirement 720/462 L 1.56 L
- Infusion rate 1.56/25 62 mL/hr (plus extra for
ongoing urinary Na output)
32
Other causes of euvolameic hyponatraemia
- Psychogenic hyponatraemia
- Massive water intake (20 - 30 L/day)
- Urine osmolality lt100 mOsm/kg
- Beer-drinkers potomania
- High volume low solute drinks impair ability to
excrete water - Hypothyroidism
- Reset osmostat
- Pure glucocorticoid deficiency
- Cortisol is required for renal free water
excretion
33
Cerebral salt wasting
- SIADH
- 1º increase in AVP
- Inappropriate urine hyperosm.
- Volume-expansion
- Suppressed aldosterone
- Appropriate natriuresis
- Decreased urea and urate
- Treatment fluid restriction
- CSW
- Cerebral damage
- Reduced SNS efferents /- BNP
- Inappropriate natriuresis
- Volume-depletion
- Volume mediated AVP release
- Appropriate urine hyperosm.
- Treatment Normal saline infusion
34
(No Transcript)
35
Case 4
- A 53-year old bachelor was brought to the AE
department having been found semi-comatose. He
was known to be a heavy drinker of alcohol. On
examination he was jaundiced. His abdomen was
distended there was hepatomegaly and evidence of
ascites. He had ankle oedema. - Serum Ref range
- Creatinine 84 µmol/L 75 120
- Urea 10.0 mmol/L 3.0 7.0
- Sodium 111 mmol/L 133 143
- Potassium 4.9 mmol/L 3.6 4.6
- Bilirubin 166 µmol/L lt 17
- Alk phos 175 U/L 21 - 92
- ALT 450 U/L 5 40
- Albumin 24 g/L 35 55
- Total protein 72 g/L 62 80
- Globulin 48 g/L 22 - 36
36
Oedematous hyponatraemia
- Splanchnic arterial underfilling / vasodilatation
- ?
- Non-osmotic release of AVP
- ?
- Impaired renal water retention
- ?
- Dilutional hyponatraemia
Recommended
CrystalGraphics Presentations





























