
Fusionless Correction for Early Onset Scoliosis (EOS) - PowerPoint PPT Presentation
Title:
Fusionless Correction for Early Onset Scoliosis (EOS)
Description:
Fusionless Correction for Early Onset Scoliosis (EOS) Emma Orton BME 281 What is EOS? Diagnosed before the skeletal age of 10 There is a lateral curve of the spine ... – PowerPoint PPT presentation
Number of Views:162
Avg rating:3.0/5.0
Title: Fusionless Correction for Early Onset Scoliosis (EOS)
1
Fusionless Correction for Early Onset Scoliosis
(EOS)
- Emma Orton
- BME 281
2
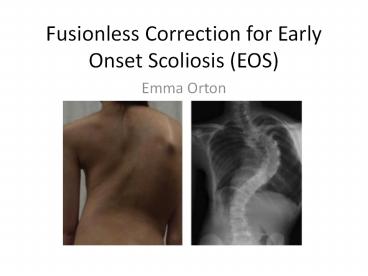
What is EOS?
- Diagnosed before the skeletal age of 10
- There is a lateral curve of the spine
- Causes pulmonary problems later in life
- There are three different types
- Infantile Idiopathic- diagnosed between 0 and 3
years old and the patient is otherwise healthy - Juvenile Idiopathic-diagnosed between 4 and 10
years old - Congenital-is developed within the first 6 weeks
of embryonic formation and is when vertebrae are
not formed correctly
1
3
Cobb Angle
2
4
3
5
Possible Treatments
- Braces
- For older patients with a less severe curve
- will not be helpful for patients aged 2-7 years
with curves of 50 to 60 degrees - VECTR
- Vertical prosthetic titanium prosthetic rib
- Pushes ribs apart widening the thorax and
straightening the spine - Dual Growing Rods
- Growing Rods with Magnetic Expansion Control
- Spinal Fusion
- Many other surgical treatments
6
Why are Fusionless Treatments Better?
- When fusion is used the curve of the spine is
improved but growth stops - Fusionless treatments are important for children
especially those under 10 - Children under 5 still have up to 12.5 cm of
vertical growth - Lungs do not fully develop till about 8 years old
- Fusion does work for patients who are fully grown
4
7
Criteria for Dual Growing Rods
- The general criteria is
- Significant potential axial growth remaining
- A deformity that is continuing to progress
- A deformity that is flexible or can be made
flexible
8
Dual Growing Rods Experiment 1
- 38 patients
- Followed for anywhere between 2 and 7 years (on
average 3.3 years) - Patients received lengthenings on average every
6.8 months - The cobb angle decreased from 74 degrees to 38
degrees on average - There was axial growth (T1-S1)
5
9
Dual Growing Rod Experiment 2
- 23 patients
- Cobb angle corrected from 82 degrees to 38
degrees on average - On average 1.24cm per year of axial spinal growth
- Improvement of space in the thorax
- 13 complications with 11 patients
10
Dual Growing Rod Experiment 3
- Group 1 had a single rod with a short apical
fusion - Group 2 had only a single rod
- Group 3 had dual rod implantation
- Group 1 had the worst results with 23 correction
(6.4cm of axial growth) while group three had the
best with 71 correction (12.1 cm of axial growth)
11
Pros and Con of Dual Growing Rod
Pros
Cons
- One of the most efficient ways of treating EOS
- Opens up the thorax preventing many future
pulmonary issues - Continues to allow for growth
- Each patient must receive an invasive surgery
every six months for a span of a few years
(usually till age 10 for girls and age 13 for
boys) - This leads to more opportunities to contract some
kind of infection - Very physically and psychologically grueling
12
Magnetically Controlled Growing Rods (MCRG)
- Attached in basically the same way as the dual
growing rods - Lengthened during quick follow-ups in the office
without any invasive surgery every 3-4 months - This allows for the curve to be managed until
their skeletal structure has matured enough for
spinal fusion - The EOS is then tracked using radiographs
6
13
7
14
MCGR
- This technique is very new in the United States
so not many hospitals are doing it - The first one was completed in Washington DC on a
ten year old boy - The requirements are a skeletal age of 10 years
old or younger and a Cobb angle of 50 degrees or
greater - Approved by the FDA in February of 2014
15
8
16
MCGR Experiment
- Criteria
- Younger than 11 years old
- Major curve of at least 30 degrees
- Radiographic thoracic height (T1-T12) less then
22cm - No previous spine surgery
- 2 year follow-up
- The Experiment
- 12 MCGR patients
- 12 TGR patients
- All paired by gender number of rods, age, curve
and type of EOS
6
17
Results
- Major Curve Correction
- Very similar with MCGR and TRG patients
- Overall it was 32 and 33
- Spinal Height(T1-S1)
- MCGR- 8.1mm/year
- TGR- 9.7mm/year
- This is not considered significantly different
- Throacic Height(T1-T12)
MCGR TRG
Height before surgery 158mm 166mm
Height immediately following surgery 186mm 189mm
Growth per year 1.5mm/yr 2.3mm/yr
18
Results
- MCRG
- 16 surgeries
- 137 noninvasive lengthenings
- 8 implant related complications
- TRG
- 73 surgeries
- 12 for initial implant
- 56 for lengthening
- 11/12 had complications
- 4 surgical site infection and 13 implant related
- NOTE All of these patient were from different
facilities so there could be some variations
in results
6
19
Discussion of Results
- MCGR-does not allow for the sagittal plane to
contour ideally because of where the actuator has
to be located - TRG-May produce better results when solely
looking at numbers but when the surgeries and
many complications are added in it is not ideal - It is possible that the MCRG would have had
results even more similar or better than the TRG
results had there been a longer follow up
(average follow up for TR patients was 1.6 years
longer)
20
References
- 1 "Congenital Scoliosis." - Scoliosis Research
Society (SRS). N.p., n.d. Web. 22 Sept. 2015. - types of scoliosis
- 2 "Anatomy of the Spine." Spine Anatomy
Southern Oregon Neurosurgical Spine Associates,
PC. N.p., n.d. Web. 26 Sept. 2015. - 3 "MD Lingo." MD Lingo. N.p., n.d. Web. 26
Sept. 2015. - 4 Hershman, Staurt H., Justin J. Park, and
Baron S. Lonner. "Fusionless Surgery for
Scoliosis." Fusionless Surgery for Scoliosis
(2013) n. pag. Web. 22 Sept. 2015. - 5 "Frequently Asked Questions." Growing Spine
- Foundation. N.p., n.d. Web. 22 Sept. 2015.
- 6 Pawlek, Jeff B., and Growing Spine Study
Group. "Traditional Growing Rods Versus
Magnetically Controlled Growing Rods for the
Surgical Treatment of Early-Onset Scoliosis A
Case-Matched 2-Year Study." 2.6 (2014) 493-97.
Web. - 7 Controlled Growing Rods Treat Scoliosis in
Children." MedGadget. N.p., n.d. Web. 22 Sept.
2015. - 8 Chueng, and Samartzis. "Management of EOS."
N.p., n.d. Web.
Recommended
CrystalGraphics Presentations





























