
Hypertriglyceridemia - PowerPoint PPT Presentation
1 / 34
Title:
Hypertriglyceridemia
Description:
... lipidemia retinalis, HSM ... other effects include reduction ... hypertriglyceridemia Primary Hypertriglyceridemia Primary Hypertriglyceridemia Clinical ... – PowerPoint PPT presentation
Number of Views:353
Avg rating:3.0/5.0
Title: Hypertriglyceridemia
1
Hypertriglyceridemia
- Jenny Shu, IM PGY-1
- November 28, 2012
2
Objectives
- To outline an approach to patients with
hypertriglyceridemia - To discuss primary and secondary causes of
hypertriglyceridemia - To discuss the non-pharmacologic and
pharmacologic therapies available for
hypertriglyceridemia
3
Definition
- Serum triglyceride (TG) concentration can be
stratified in terms of population percentiles
and/or coronary risk - Normal 1.7 mmol/L
- Borderline high 1.7 to 2.2 mmol/L
- High 2.3 to 5.6 mmol/L
- Very high 5.7 mmol/L
4
Sources of plasma TG
- Exogenous
- From dietary fat
- After meal gt 90 circulating TG originate in
intestine, secreted in CMs - Endogenous
- From liver
- During fasting, secreted by liver as VLDL
predominate hydrolyzed by LPL ? free FA
5
Lipid metabolism
- High TG because of either
- Increased production from liver and intestine
(upregulated synthetic and secretory pathways) - Decreased peripheral catabolism reduced LPL
activity
6
Why do we care?
- Hypertriglyceridemia has implications for
- Cardiovascular disease
- Directly
- Indirectly
- Pancreatitis
- Cerebrovascular disease
7
Incidence
- In US National Health and Nutrition Examination
Surveys (NHANES) from 1999 to 2004 - adults with TG gt 1.7mmol/L 33
- TG gt 2.3 mmol/L 18
- TG gt 5.7 mmol/L -1.7
- TG gt 11.3 mmol/L 0.4
Data from Genest JJ, McNamara JR, Ordovas JM, et
al. J Am Coll Cardiol 1992 19792.
8
Types of hypertriglyceridemia
- Primary (inherited)
- Familial chylomicronemia (type I)
- Primary mixed hyperlipidemia (type V)
- Familial hypertriglyceridemia (type IV)
- Familial combined hyperlipoproteinemia (type IIB)
- Familial dysbetalipoproteinemia (type III)
- Secondary (acquired)
- Medications or exogenous substances
- Other medical conditions
9
Primary Hypertriglyceridemia
- Familial chylomicronemia (I) primary mixed
hyperlipidemia (V) - Both associated with pathologic presence of CMs
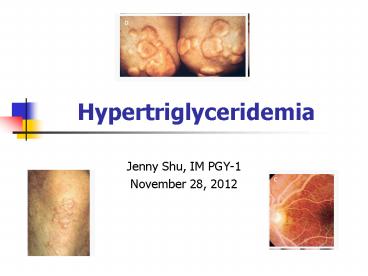
after 12-14h period of fasting - Clinical features include eruptive xanthomata,
lipidemia retinalis, HSM, focal neurological
deficits (irritability), recurrent epigastric
pain (pancreatitis risk) - Typically plasma TG gt 10 mmol/L
10
Primary Hypertriglyceridemia
- Familial chylomicronemia (I) vs primary mixed
hyperlipidemia (V) - Timing of onset
- Biochemically proven deficiencies in LPL, apo CI
activity or homozygous gene mutations - Secondary factors
- Greater elevation of total cholesterol
11
Clinical Manifestations
Lipemia retinalis usually TG gt 35 mmol/L
Eruptive cutaneous xanthoma trunk, buttocks,
extremities
Palmar crease xanthomas Type III
Tuberous xanthomas extensors, usually Type III
Yuan G et al. CMAJ 20071761113-1120
12
When draw blood, you will see
- Creamy supernatant when refrigerated overnight
- (4 degrees C)
Yuan G et al. CMAJ 20071761113-1120
13
Primary Hypertriglyceridemia
- Mixed hypertriglyceridemia (Type IV)
- Isolated elevation VLDL (not as TG rich as CMs),
5-10 population prevalence - Likely polygenic
- Mod elevated plasma TG (3-10 mmol/L)
- Low levels HDL-C
- Increased risk CAD, obesity insulin resistance,
DM, htn, hyperuricemia
14
Primary Hypertriglyceridemia
- Familial dysbetalipoproteinemia (type III)
- Increase in TG rich lipoprotein remnants IDL or
beta-VLDL that produce equimolar elevation plasma
total cholesterol and TG - Population prevalence 1-2 in 20 000
- Usually homozygotic for binding defective APOE E2
isoform phenotypic expression often requires
other RF such as T2DM, obesity, or hypothyroidism - Also with elevated LDL (interrupted processing
VLDL) diagnostic when high VLDL-C TG ratio
with E2/E2 homozygosity - Increased risk cardiovascular disease, often have
tuberous/tuberoeruptive xanthomata on extensor
surfaces
15
Primary Hypertriglyceridemia
- Familial combined hyperlipoproteinemia (Type IIB)
- Increased VLDL and LDL, low HDL
- Autosomal dominant with variable penetrance, 2-5
population prevalence - At least one 1st degree relative with abn
lipoprotein profile - Affected individuals usually obligate
heterozygosity for LPL or APO3 gene mutation, but
unknown molecular basis in most cases, other
genes implicated include USF1, APOA5, APOC3
16
Secondary Hypertriglyceridemia
- Other medical conditions
- Renal disease
- Usually ass. With high LDL-C
- Nephrotic syn ass high apo B containing
lipoproteins such as VLDL - Obesity/metabolic/DM
- Excess adipose tissue high TG, low HDL-C
- Part of metabolic syndrome
- NASH
- High TG, low HDL-C are defining components
- Statin treatment may be more effective than
fibrates
17
Secondary Hypertriglyceridemia
- Other Medical conditions
- Pregnancy during T3, plasma TG can go up to 3x
normal - Minimal clinical consequence
- Should not always assume due to pregnancy can
get chylomicronemia (rare) ? complicated
pancreatitis serious health consequences for
mother and fetus - Other
- Sedentary lifestyle
- Diet positive energy intake balance and high
fat/GI - Paraproteinemias e.g hypergammaglobuliemia in
macroglobulinemia, yeloma, lymphoma, lymphocytic
leukemias), autoimmm (SLE)
18
Secondary Hypertriglyceridemia
- Medications or Exogenous Substances
- Medications
- Steroids, estrogens (esp po), tamoxifen, anti-htn
(non cardioselective BB, thiazides),
isotretinoin, bile acid-binding resins,
cyclophosphamide, antiretroviral regiemns
(HAART), psychotropic (phenothiazines, 2nd gen
anti psychotics) - Alcohol
- Due to high VLDL /- chylomicronemia
- Can have normal TG because of adaptive increase
in lipolytic activity
19
Approach to Management
- IF TG gt 10 start FIBRATE right away
- Then lifestyle, rule out secondary causes,
dysglycemia - If TG 4.5 10,
- Lifestyle intervention, rule out secondary causes
- Address dysglycemia
- Fibrate, ezetimibe, niacin
- If TG 2 4.5,
- Lifestyle intervention, rule out secondary causes
- Address dysglycemia
- If patient already on statin, can intensify
statin dose - Or can try any of fibrate, niacin, fish oil,
ezetimibe
Yuan G et al CMAJ 20071761113-1120
20
Conservative Management
- Non-pharmacological
- Conservative measures such as weight reduction,
diet modification, exercise - Goal for dieting is to decrease wt overall intake
of energy/fat/refined carbs (high GI) - Fat intake should be 10-15 total energy intake
(15-20 g/d) if severe hypertriglyceridemia - Avoid alcohol
- Underlying cause hypothyroid, renal disease
etc. - Better glycemic control of DM
- Omega-3 FA component of Mediterranean diet and
fish oils - Daily consumption 4g restricted energy and
saturated fat intake can reduce TG by 20 - Rarely effective when sole TG-lowering therapy
21
Pharmacologic agents
- Fibrates
- Mainstay of treatment, generally well tolerated
(rare hepatitis/myositis), other effects include
reduction of LDL, increase HDL-C activates
PPAR-alpha to activate LPL action inducing
lipolysis and elimination of TG rich particles - Statins
- Inhibit HMG-CoA reductae, not 1st line with TG gt5
mmol/L as monotherapy - Safety profile appropriate combo with fibrate as
FIELD showed no rhabdomyolysis among more than
1000 patients taking combination statin
fenofibrate - Niacin (daily consumption up to 3g)
- Binds GPCR and inhibits adipose breakdown,
decreases VLDL, increases HDL, lowers TG up to
45, start low gradually increase - Other lipid lowering medications
- Ezetimibe inhibits cholesterol absorption, safe
in combo with fibrates - Emerging treatments
22
Efficacy of Various Agents
- Fibrates 10-50 ?TG
- Ezetimibe 10-15 ?TG
- Statins 7-30 ?TG
- Niacin 20-50 ?TG
- Omega-3 fatty acids 15-20 ?TG
23
Evidence for Omega-3
- Contain EPA and DHA dose dependent TG lowering
effect through various mechanisms decreased
VLDL secretion, improved VLDL TG clearance - JELIS trial (Yokoyama et al Lancet 2007 369
1090-8) found 1.8g/d EPA supp low dose statin
decreased rate major coronary events compared
statin monotherapy (? Related to TG since minimal
reduction in levels (reduction 9 from baseline
in EPA group vs. 4 in controls) plt00001 - GISSI-P (Lancet 1999 354, 447-455) showed 1g/d
as 1 cap Omacor reduced all cause mortality and
sudden death in patients with previous MIs - Benefit on mortality?
- Recent JAMA systematic review and meta-analysis
2012 (Rizo et al) ? overall, omega-3 PUFA
supplementation was not associated with a lower
risk of all-cause mortality, cardiac death,
sudden death, myocardial infarction, or stroke
based on relative and absolute measures of
association - Did not support that higher TG lowering dose was
more protective than lower TG lowering dose
24
Fibrates
- Fenofibrate most commonly prescribed
- Lipidil EZ 145 mg od
- Lipidil (fenofibrate) supra 160 mg od
- Fenofibrate 200 mg od
- Gemfibrozil (lopid) 600-1200 mg od
- Bezafibrate (bezalip) 400 mg od
25
Safety concern with fibrates
- Baseline and post-initiation
- CK, creatinine, INR (if receiving anti-coagulants
potentiates actions) risk myalgias, myopathy,
rhabdomyolysis - If using in combination with statin, fenofibrate
recommended (lower risk rhabdo) - Be aware of implications of renal dysfunction
- Up to 15-20 increase in Cr acceptable, but may
need to dose reduce - Potential increased risk for cholelithiasis
(clofibrate), follow LFTs
Davidson MH et al Am J Cardiol 200799(6A)3C-18C
26
Evidence for fibrates
- Meta-analysis looked at 6 RCTs, showing fibrate
Tx significantly reduced subsequent vascular
event risk and effective in lowering TG levels - FIELD
- ACCORD-Lipid
Lee M et al Atherosclerosis 2011217492-498
27
Meta-analysis Fibrates CVD
Trial (drug) population of patients with diabetes Primary endpoint entire cohort (p value) Lipid subgroup criterion Analysis(p value)
HHS (gemfibrozil) 4081 (100 male) 3 -34 (0.02) TG gt 2.26 mmol/L LDL-C/HDL-C gt 5.0 Post-hoc -71 (lt0.005)
VA-HIT (gemfibrozil) 2531 (100 male) 25 -22 (0.006) TG 1.69 mmol/L Post-hoc -27 (0.01)
BIP (bezafibrate) 3090 (91 male) 10 -7.3 (0.26) TG 2.26 mmol/L Post-hoc -39.5 (0.02)
FIELD (fenofibrate) 9795 (63 male) 100 -11 (0.16) TG 2.30 mmol/L HDL-C lt 1.086 mmol/L Post-hoc -27 (0.005)
ACCORD (fenofibrate) 5518 (69 male) 100 -8 (0.32) TG 2.30 mmol/L HDL-C 0.879 mmol/L Prespecified -31 (0.06)
28
Evidence for fibrates meta analysis
Lee M et al Atherosclerosis 2011217492-498
29
FIELD
- Studied effect of fenofibrate on cardiovascular
disease events in DM patients (not taking statin
at entry) - Allocation to fenofibrate (200 mg daily) resulted
in reductions relative to placebo in plasma
total-cholesterol concentration of 11,
LDL-cholesterol level of 12, and TG of 29, and
increases in levels of HDL cholesterol of 5
after 4 months of treatment. - However no statistically significant reduction in
combined outcome of all-cause mortality and non
fatal MIs despite reducing TGs - Did show reduction in non-fatal MI and coronary
revascularization rate in fenofibrate arm,
reduction microvascular complications of DM,
reductions proteinuria and laser eye
interventions
FIELD Lancet 20053661849-1861
30
FIELD
FIELD Lancet 20053661849-1861
31
ACCORD-Lipid
- Whether combination therapy with a statin
(simvastatin) plus a fibrate (fenofibrate) vs.
statin alone reduces cardiovascular risk in T2DM
patients at high risk - Median plasma triglyceride levels decreased from
1.85 to 1.38 mmol/L in fenofibrate group and from
1.81 to 1.63 mmol/L in placebo group - Conclusion was that combo fenofibrate and
simvastatin did not reduce the rate of fatal
cardiovascular events, nonfatal myocardial
infarction, or nonfatal stroke, as compared with
simvastatin alone - However pre-specified subgroup with TG gt11.3
mmol/L and HDL lt 1.89mmol/L could benefit due to
improvement of primary outcome (p 0.057) - FDA May 2011- trial not designed for mixed
dyslipidemia, inappropriate to infer combo
therapy ineffective
ACCORD LIPID NEJM 20103621563-1574
32
ACCORD-Lipid
ACCORD LIPID NEJM 20103621563-1574
33
Conclusion
- Classify hypertriglyceridemia based on severity
moderate RF for cardiovascular/CVS disease,
severe RF for pancreatitis - When thinking about etiology, consider primary
vs. secondary causes - Based on severity, consider non-pharmacological
and pharmacological Tx and dont forget about
safety profile - Needs to be more high-powered RCTs looking at
combination therapy and cardiovascular outcomes
34
Discussion/Questions
- Thanks for your attention.
Recommended
CrystalGraphics Presentations





























