
48x36 Poster Template - PowerPoint PPT Presentation
1 / 1
Title:
48x36 Poster Template
Description:
Non-authorized printing of this poster template by any commercial printing service other than PosterPresentations.com is strictly prohibited. Non-profit educational ... – PowerPoint PPT presentation
Number of Views:145
Avg rating:3.0/5.0
Title: 48x36 Poster Template
1
In children under the age of five, is bracing as
effective as surgery at correcting Blount's
disease (tibial varum) and preventing future
musculoskeletal impairments? Kristin Hamrick
Brandy Hirsch Bellarmine University DPT Class of
2015
Classification
Non-operative Intervention
Background
Outcomes Conclusion
- Surgery
- Potential motor weakness and/or sensory deficits
secondary to damaged fibular nerve 5 - Not recommended before age 2 5
- Definitive surgery for infantile Blount's
disease is most successful before age 5 to
prevent recurrence 2 - The use of external fixation has better outcomes
than internal fixation 2 - Good prognosis if under age 3, normal weight,
Langenskiold stage I or II, ADA angle lt 18 6 - MPS most significant MPS angle or lt 59
degrees 6 - Bracing
- Bracing appears to be effective in stages I II
infantile Blount's disease, specifically in cases
with unilateral involvement 3 - Children with bilateral disease or age greater
than 4 are more likely to require surgical
intervention 3 - Research suggests that daytime, ambulatory
bracing can correct tibial vara in patients lt 3
years of age 7 - Overall, outcome depends on patients age and
severity of deformity at the time of intervention
3 - Ultimately, if implemented early, bracing is an
effective and less invasive treatment for
Blounts disease, especially infantile form
stages I II 8
- Blounts Disease
- Uncommon growth disorder usually seen in
children and adolescents as a result of internal
rotation of the proximal tibia immediately below
the knee - Although Blounts disease is idiopathic,
biomechanical factors are still considered to be
a large contributor of the pathological cycle 7 - Presents as excessive varus angulation at the
knee - Progressive (gets worse, not better) 1
- 3 Categories 2
- 1. infantile tibia vara before 4 years of age
- Typically bilateral
- MD angle gt 16 degrees
- 5x more common than adolescent form
- 2. juvenile tibia vara between 4-10 years
- 3. adolescent tibia vara after 10 years
- Typically unilateral
- Associated clinical characteristics 1,3,6
- Early walkers
- Obese
- African Americans
- Langenskiold Classification six roentenographic
stages depending on degree of skeletal maturation
and upper end bone development 4 - I under 3 yrs., medial and distal beaking of
metaphysis with irregularity of entire metaphysis - II age 2.5-4 yrs., sharp anteromedial
depression and ossification line of wedge-shaped
medial metaphysis - III age 4-6 yrs., deepening of metaphyseal beak
- IV 5-10 yrs., enlargement of epiphysis
- V 9-11 yrs., cleft in epiphysis, appearance of
double epiphysis - VI 10-13 yrs., closure of medial proximal
tibial physis - Catonne Classification six stages based on
progressive radiographic change 4 - I 2-3 yrs., asymmetry of tibial epiphysis
- II 3-5 yrs., sloped epiphysis uneven
metaphyseal shape - III 5-8 yrs., vertical medial epiphysis and
metaphysis, medial calcifications - IV 8-11 yrs., small medial bony bridge
- V medial bony bridge
- VI adult aspect of physis
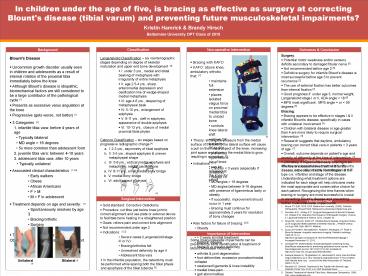
- Bracing with KAFO
- KAFO above knee, ambulatory orthotic that 7
- maintains full extension
- places isolated valgus force on proximal medial
tibia to unload bone - controls knee lateral shift
- allows DF but limits PF to 90
- prevents hyperextension of knee
- can be released at the knee for sitting
- Theory shifting the pressure from the medial
surface of the tibia to the lateral surface will
cause a pull on the medial aspect of the knee,
increasing joint space and allowing the medial
tibia to grow, resulting in correction. 7 - Indications 3,7
- Children lt 3 years (especially if unilateral)
- Stages I-II
- MD angles gt 16 degrees
- MD angles between 9-16 degrees with presence of
ligamentous laxity or obesity - If successful, improvement should occur in 1
year - Bracing must continue for approximately 2 years
for resolution of bony changes - Risk factors for failure of bracing 3,8
- Obesity
- Varus thrust
- gt 3 years at initial treatment
- Bilateral disease
- Stage III or greater deformity
7
Clinical Relevance
The key to successful treatment of Blounts
disease in the clinic is early identification of
the type (i.e. infantile) and stage of the
disease. Understanding what treatment options are
indicated for each stage will help clinicians
make the most appropriate and conservative choice
for each patient. Recognizing the time frames
when bracing or surgery are most successful is
crucial in correcting Blounts disease and
preventing further musculoskeletal impairments.
4
Surgical Intervention
Literature Cited
- Gold standard Corrective Osteotomy
- Procedure cut tibia just below knee joint to
correct alignment and use plate or external
device to facilitate bone healing in a
straightened position - Goals relieve pain and correct limb alignment
- Not recommended under age 2
- Indications 1,2
- Severe cases (Langenskiöld stage III or IV)
- Bracing/orthotics fail
- Unresolved deformity by age 4
- Adolescent tibia vara
- In the infantile population, the osteotomy must
be performed while sparing both the tibial physis
and apophysis of the tibial tubercle 3
- Boyce PT, EdD, OCS, ECS. Bellarmine University.
(2009). Pediatric Orthopedics. PowerPoint.
Retrieved by blackboard.bellermine.edu - Davidson R.S., Shirley E.D. Surgical Management
of Blount's Disease. Inc Wiesel S.W. Operative
Techniques in Orthopaedic Surgery. Volume II.
Lippincott Williams Wilkins 2012 Chapter 30. - Doyle BS, Volk AG, Smith CF. Infantile Blount
disease long-term follow-up of surgically
treated patients at skeletal maturity. J Pediatr
Orthop. Jul-Aug 199616(4)469-76. Medline. - Ducou le Pointe H, Mousselard A, Rudelli A,
Montagne J.P, Filipe G. Blount's disease
magnetic resonance imaging. Pediatric radiology.
19952512-14. http//link.springer.com/article/10
.10072FBF02020831page-1 Accessed November 15,
2013. - Jahangiri FR. Multimodality neurophysiological
monitoring during tibial/fibular osteotomies for
preventing peripheral nerve injuries. The
Neurodiagnostic journal. 201353(2)15368.
Available at http//www.ncbi.nlm.nih.gov/pubmed/2
3833842 - Kaewpornsawan K, Tangsataporn S, Jatunarapit R.
Early proximal tibial valgus osteotomy as a very
important prognostic factor in Thai children with
infantile tibia vara . Journal of the Med
Association of Thailand. 2005572-79. - Marshall JG. Orthotic Treatment of the Toddler
with Bowed Legs. Pediatric Portal. Nov 2010 4-6.
OP Business News. - Orthotic Treatment of Infantile Tibial Vara.
Medscape Orthopedics. 1999 3(6)
www.medscape.com
Importance of Intervention
- Some musculoskeletal impairments can be prevented
by early identification treatment of Blounts
disease, including - arthritis joint degeneration
- foot deformities excessive pronation/medial
collapse - weakened ligaments knee instability
- medial knee pain
- gait abnormalities
Bilateral 1
Unilateral 1
Recommended
CrystalGraphics Presentations





























