
ECG Interpretation - PowerPoint PPT Presentation
1 / 53
Title: ECG Interpretation
1
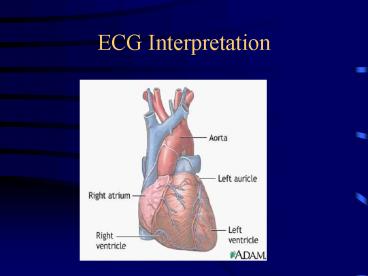
ECG Interpretation
2
What is an ECG
- Electrocardiogram
- Traces the electrical activity of the heart
- 12 lead, 15 lead
3
Uses of ECG Tracing
- Ischemia/infarct
- Arrhythmias
- Ventricular and atrial enlargements
- Conduction defects
- Pericarditis
- Effects of some drugs and electrolytes
4
ECG
5
How to Conduct an ECG
- Patient lies flat on back
- Electrodes are placed on the body
- Sites may need to be shaved or cleaned to ensure
the leads will stick properly. - Patient will lie as still as possible, hold
breath, or put hands under bottom to keep from
moving. - The results are then printed out on paper for MD
to review.
6
ECG Strip
7
Lead Placements
- V1 - Junction of the 4th ICS, Right sternal
border - V2 - Junction of the 4th ICS, Left sternal border
- V3 - Midway between V2 and V4
- V4 - Junction of 5th ICS, Mid clavicle
- V5 - Anterior aspect of axilla, same line as V4
- V6 - Mid axilla, same line a V4
- 4 limb leads (for grounding etc)
8
Lead Placements Cont
9
(No Transcript)
10
Normal Conduction Pattern
11
Understanding the Waves
12
Each wave
- P
- Q
- R
- S
- T
13
(No Transcript)
14
ECG Strip r/t heart
15
Understanding the Waves
- One small box 0.04 seconds
- One large box 0.2 seconds
- 5 large boxes 1 second
16
http//en.wikipedia.org/wiki/FileECG_principle_sl
ow.gif
17
Understanding the Waves
- Baseline (what is it?)
- P wave
- Length of time it takes the impulse to pass from
the SA node to the AV node - Should precede every QRS wave
- PR interval
- Should be no longer than 0.12 0.2
18
Understanding the Waves
- QRS
- Should be no longer than 0.12
- If energy is going towards a positive electrode
(camera), the picture will show a positive QRS
complex - If energy is going away from positive electrode,
the picture will show a negative QRS complex - If energy is toward the positive electrode and
then passes by it, the QRS will be biphasic - Ventricle contracting
19
Understanding the Waves
- T wave
- Should always start from baseline
- Will indicate ischemia
20
Understanding an ECG
- Is as easy as
- 1.
- 2.
- 3.
- rate
- intervals
- rhythm
21
Step 1 Rate
- Different ways to calculate a rate
- a) ECG usually tells you
- b) Locate a QRS that is close to a big line and
count to next big line 300, 150, 100, 75, 60, 50 - c) take a 6 second strip, count QRS and multiply
by 10 (hint the middle of V3 on the lead II
strip is 6 seconds)
22
Step 1 Rate (cont)
- Checking the regularity
- map out QRSs
23
Step 2 Intervals
- We assess intervals to see where the impulse is
coming from (pacemaker beat) - Remember
- PR interval normal is 0.12 - 0.2
- QRS interval normal is less than or equal to
0.12
24
Step 3 Rhythm
- The biggest question in relation to rhythm is
25
- Is this rhythm affecting my patient?
26
(Normal) Sinus Rhythm
- 60-80 bpm
- P preceding each QRS
- Normal intervals
27
Normal ECG
28
Other Sinus Rhythms
- Sinus bradycardia
- a sinus rhythm with a rate lt60 bpm
29
Other Sinus Rhythms
- Sinus tachycardia
- a sinus rhythm with a rate gt80 bpm
30
Atrial Arrhythmias
- Atrial fibrillation (A-fib)
- irregular rate
- no discernable P waves
- increased risk of strokes due to clots that might
form due to fibrillation (patients are usually on
anticoagulation therapy)
31
Atrial fibrillation
32
Atrial Arrhythmias Cont
- Atrial flutter
- saw tooth in appearance
- irregular rate
33
Atrial flutter
34
Blocks
- 1st degree AV block
- a PR interval that exceeds 0.20 sec
35
Blocks Cont
- 2nd degree AV block (Mobitz)
- a) type I (Wenckebach)
- longer and longer PR intervals until a QRS is
dropped
36
Blocks Cont
- b) type II
- P waves and then suddenly a QRS is dropped
- Ps are regular
37
Blocks Cont
- 3rd degree AV block
- HR lt40 bpm
- a complete block of electrical activity from
atria to ventricle - Ps are regular
38
Ventricular Rhythms
- Ventricular fibrillation
- complete breakdown of all rhythm
- a) course
- b) fine
39
V-fib
- Whats the first thing to do when coming up on a
patient with this rhythm?
40
Ventricular Rhythms Cont
- Ventricular tachycardia (V-tach)
- impulse originates in the ventricle
- always has a wide QRS complex
41
V-tach Whats the first thing to do when coming
up on a patient with this rhythm?
42
Asystole
- Pulseless
43
Coronary Arteries
44
MIs
45
MIs
46
MIs
- How can you tell on an ECG that your patient is
having a heart attack? - T waves
- Different views of heart will show different
injured areas of heart
47
MIs
- T wave shouldering is classic
48
MIs
- How else can you tell that your patient has had
an MI? - Cardiac Markers
- CK will show in 4-6 hours (starts to come back
down after 1 day) - Troponin will show in 4-6 hours (may stay
elevated for weeks) - Others are LDH, CK-MB, myoglobin, AST
49
Locating an MI
50
I Lateral (circumflex) aVR V1 Anterior (Lt ant desc) V4 Anterior
II Inferior (Rt coronary) aVL Lateral V2 Anterior V5 Lateral
III Inferior aVF Inferior V3 Anterior V6 Lateral
51
ECG Tissue Damage Locations
52
(No Transcript)
53
Where is this MI?
Recommended
CrystalGraphics Presentations





























