
Helical CT Screening for Lung Cancer at Advanced Radiology Consultants - PowerPoint PPT Presentation
1 / 25
Title:
Helical CT Screening for Lung Cancer at Advanced Radiology Consultants
Description:
Helical CT Screening for Lung Cancer at Advanced Radiology Consultants Lung cancer missed on CXR Why screen for lung cancer? Lung cancer is a major health problem It ... – PowerPoint PPT presentation
Number of Views:155
Avg rating:3.0/5.0
Title: Helical CT Screening for Lung Cancer at Advanced Radiology Consultants
1
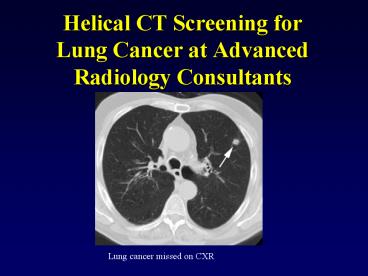
Helical CT Screening forLung Cancer at Advanced
Radiology Consultants
Lung cancer missed on CXR
2
Why screen for lung cancer?
- Lung cancer is a major health problem
- It is the most common cause of cancer death in
men and women in the United States - Approximately 160,400 patients will die as a
result of the disease over the course of the next
year
3
Why screen for lung cancer?
- Overall survival for lung cancer is presently
very poor- 5 year survival is about 15 - Most patients present with advanced disease-
regional spread in 29 and distant spread in 52
Advanced stage lung cancer at presentation
4
Why screen for lung cancer?
- Lung cancer prognosis depends on stage at
presentation - Patients with Stage IA lesions (less than 3 cm in
size and no lymph node or distant metastases)
have a 5 year survival of 67 to 80 - Therefore, want to identify patients with early
stage lung cancer in an attempt to improve long
term survival
5
Why screen for lung cancer?
- CXR screening is not recommended, but physicians
will order yearly CXR's on their patients-
particularly smokers or ex-smokers - A conservative estimate is that about 50 of
cancers will go undetected on the patient's
initial CXR - Studies have demonstrated that helical CT is
clearly superior to CXR for the identification of
small pulmonary nodules
6
Small Lung Cancer Missed on CXR
Where is the cancer? Note small granuloma in left
apex.
7
Lung Cancer Missed on CXR- Stage IIA
Cancer cannot be definitively seen on CXR even
retrospectively
8
BIG Lung Cancer Missed on CXR- T4 lesion
Large cancer missed on CXR (luckily not by ARC
physician)
9
Helical CT Screening Studies Summary
- Low dose helical CT is clearly superior to CXR
for the detection of early stage lung cancer - Between 60-90 of cancers detected on low dose CT
are Stage IA lesions - CXR fails to detect a lesion in about 75 of
these patients - Early detection of Stage I lung cancers will lead
to overall improved lung cancer survival (I-ELCAP
conclusion)
10
Positive lung screen CT scan
- Patient had screen in 2002, lost to follow-up
- Primary HCP sent patient for repeat screening
exam in 2007- positive for small lung cancer
2002
2007
11
Helical CT Screening the Controversy
- Survival ? Mortality
- Screening improves survival, but does screening
decrease mortality?
12
JAMA 2007 Bach PB, et al. Computed tomography
screening and lung cancer outcomes. 297 953-961
- Screened patients were diagnosed with lung cancer
in far greater numbers than would have occurred
in the absence of screening and the majority
(67) were stage I or stage II - However, there was no decrease in overall
mortality based upon predicted models
13
Bach PB, et al. Limitations
- Lacked non-screened comparison group
- Mortality estimates used in the study depend on
the validity of prior risk factor analyses- these
may not be applicable - Because of the small number of patients in the
Bach study, the 95 confidence interval for their
data might allow for a lung cancer mortality
reduction as large as 30 - Therefore- no conclusive data regarding mortality
yet published
14
Survival and Mortality
- Other screening exams have not been shown to have
effect on mortality - Although in widespread use, prostate cancer
screening is not yet validated as providing a
clear benefit in terms of reducing mortality from
prostate cancer
15
Helical CT Screening Limitations
- Missed cancers
- False positives- non-calcified granulomas
- Interval cancers between scans
- Radiation
16
Helical CT Screening Limitations
- Lung cancers will be missed- up to 50 of cancers
will not be detected on the patients initial
screening exam - Highlights need for patient follow-up
- Good news is missed lesions are less than 1 cm
and typically ground-glass in character
(bronchoalveolar cell carcinoma)
17
Helical CT Screening Limitations
- Lesions that are missed on initial screening will
be detected on follow-up exams and are generally
Stage I - NOTE CXR detects none of these lesions
18
Missed Cancer on Screening CT
1993
1995
Bronchoalveolar cell cancer
19
Helical CT Screening Study Limitations
- False positives- non-calcified nodules are
detected in a large number of screened patients,
but only about 1-2 of these nodules prove to be
malignant - CT cannot achieve perfect discriminatory
performance- cannot 100 reliably conclude a
lesion is malignant based upon its appearance - Small nodules require follow-up and this can lead
to patient anxiety
20
Helical CT Screening Study Limitations
- A negative screen does not preclude the
subsequent development of lung cancer, even
between scans- although a rare occurrence
Highly advanced lung cancer developed over only
10 months
21
Helical CT Screening Limitations
- Scan involves use of radiation
- ARC uses a low dose technique
- Radiation exposure is approximately 10 times
higher than a CXR, but is only one-sixth that of
a conventional CT - Remember- scan provides about 10 times the
information of a standard CXR
22
Screening for lung cancer- The challenge
- KEY TO SUCCESSFUL SCREENING Must identify the
proper subset of patients that will most benefit
from screening - Best candidates are smokers (present or ex) with
20 pack year smoking histories - We are happy to discuss the scan with you or any
patient that expresses an interest in lung cancer
screening
23
Why we need to screen
Where is the cancer?
24
Why we need to screen
Stage IA cancer that cannot be seen on CXR
25
Why we need to screen for lung cancer
The annual number of deaths from lung cancer is
greater than the numbers of deaths from breast,
colon, and prostate cancer combined
Recommended
CrystalGraphics Presentations





























