
Efficacy Evaluation - PowerPoint PPT Presentation
1 / 1
Title:
Efficacy Evaluation
Description:
Empirical use of teicoplanin versus vancomycin in febrile neutropenic patients at high risk for gram-positive bacteraemia: results of a multi-centre prospective ... – PowerPoint PPT presentation
Number of Views:54
Avg rating:3.0/5.0
Title: Efficacy Evaluation
1
Empirical use of teicoplanin
versus vancomycin in febrile neutropenic patients
at high risk for gram-positive bacteraemia
results of a multi-centre prospective randomized
clinical trial 1H. Akan, 2V. Korten, 3Z. Bolaman,
4I. Aydogdu, 5G. Alanoglu, 6V. Hazar, 7T. Fen,
8Z. Gulbas, 9M. Akova (Turkish Febrile
Neutropenia Study group)
Replace with logo
Abstract
Methods
Results
Objectives To evaluate the efficacy and safety
of empirical use of teicoplanin versus vancomycin
in febrile neutropenic patients at high risk of
gram positive bacteraemia. Methods A total of
190 febrile neutropenic patients from 21 centers
were randomized to receive either teicoplanin (97
patients) or vancomycin (93 patients) in addition
to a standard empirical regimen of intravenous
ceftazidime and amikacin for a duration of 5 to
21 days, depending on response to the
treatment. Results There was no difference
between teicoplanin and vancomycin groups in
terms of overall survival rates (92.55 vs.
92.56, pgt0.05) and response rates (55.7 vs.
53.3, pgt0.05). Gram positive isolates (62.8)
from peripheral blood cultures were more than
Gram negative isolates. The adverse events
observed were not significantly different between
the two groups most common ones being
hypokalemia, eruption, diarrhea, and
hepatotoxicity. Conclusion Teicoplanin is as
effective as vancomycin in terms of treatment
response and overall survival rate in febrile
neutropenic patients. Both antibiotics have
acceptable safety profiles.
- Evaluation criteria
- Primary evaluation criteria
- Overall survival of patients during follow-up
period - Treatment response rates
Last conditions of the patients and the condition
of the underlying disease in the follow-up
evaluation are given in Table 2 for both
randomization arms.
- Body temperature, leukocyte count, ANC, ECOG
performance status, symptoms of infection,
changes in clinical focus and microbiological
data were also analyzed.
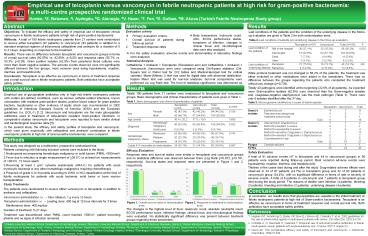
Table 2. Last conditions of patients and
underlying disease in the follow-up evaluation.
Teicoplanin (n97) Vancomycin Total (n190) P
Last condition of the patients Still in the hospital 36 (37.1) 32 (35.2) 68 (36.2) 0.832
Last condition of the patients Discharged 51 (52.6) 52 (57.1) 103 (54.8)
Last condition of the patients Dead 7 (7.2) 4 (4.4) 11 (5.9)
Last condition of the patients Other 3 (3.1) 3 (3.3) 6 (3.2)
Last condition of underlying disease Remission 21 (75.0) 19 (73.1) 40 (74.1) NA
Last condition of underlying disease Refractory 4 (14.3) 4 (15.4) 8 (14.8)
- For the safety evaluation, adverse events and
abnormalities in laboratory findings were
analyzed. - Statistical Analysis
- Ceftadizime Amikacin Teicoplanin (Teicoplanin
arm) and Ceftazidime Amikacin Vancomycin
(Vancomycin arm) were compared using Chi-Square
statistics (Chi-Square test or Fisher test for
2X2 tables and Mantel-Haenzsel test for ordinal
variants). Mann-Whitney U test was used for
digital data with abnormal distribution. Kaplan
Meier test was used for survival analyses.
Survival comparisons were performed via Log Rank
test. The level of statistical significance was
determined as plt0.05.
While protocol treatment was not changed in 58.2
of the patients, the treatment was either
switched or other medications were added in the
remainders. There was no difference between the
groups regarding the patients who completed the
treatment without any change (p0.726). Totally
43 pathogens were identified at the beginning
(22.6 of all patients). As expected more
Gram-positive isolates (62.8) were observed than
the Gram-negative isolates and,
coagulase-negative staphylococci was the main
pathogen (Table 3). There were only 6 isolates
identified after the 3rd day.
Results
Introduction
Totally 190 patients from 21 centers were
randomized to teicoplanin and vancomycin groups.
Basic demographic and clinical characteristics of
patients were given in Table 1. Table 1. Basic
demographic and clinical characteristics of
patients
Empirical use of glycopeptide antibiotics only in
high risk febrile neutropenic patients with
certain pre-defined conditions, such as serious
catheter-related infections, known colonization
with resistant gram-positive strains, positive
blood culture for gram-positive bacteria,
hypotension or other evidence of septic shock was
recommended in 2002 guidelines of Infectious
Diseases Society of America (IDSA) and the
European guidelines (i.e. ECIL-1) 1,2.
Vancomycin and teicoplanin are the main
glycopeptide antibiotics used in treatment of
beta-lactam resistant Gram-positive infections.
In comparative studies vancomycin and teicoplanin
were reported to have similar clinical and
bacteriological response rates 3. In the
present study, the efficacy and safety profiles
of teicoplanin and vancomycin, which were given
empirically with ceftazidime and amikacin
combination in febrile neutropenic patients at
high risk of Gram-positive bacteraemia, were
compared.
Table 3. Microorganisms identified as a cause of
febrile episode
Teicoplanin(n97) Vancomycin(n93) Total(n190) p value
Sex Female 42 (43.3) 42 (45.2) 84 (44.2) 0.796
Sex Male 55 (46.7) 51 (54.8) 106 (55.8)
Age (years) Age (years) 36.4 ? 20.2 37.5 ? 19.9 - 0.690
Diagnosis Hematologic malignancy 86 (93.5) 80 (96.4) 166 (94.9) 0.502
Diagnosis Solid tumor 6 (6.5) 3 (3.6) 9 (5.1)
Hematologic malignancy status Remission 52 (60.5) 44 (55.0) 96 (57.8) 0.747
Hematologic malignancy status Relapse 20 (23.3) 20 (25.0) 40 (24.1)
Hematologic malignancy status Progression 14 (16.3) 16 (20.0) 30 (18.1)
Grade II-IV mucositis at randomization Grade II-IV mucositis at randomization 34 (35.1) 31 (34.1) 65 (34.6) 0.887
Teicoplanin Vancomycin Total
Gram (-) isolates Escherichia coli 4 7 11
Gram (-) isolates Pseudomonas aeruginosa 3 0 3
Gram (-) isolates Klebsiella pneumoniae 1 0 1
Gram (-) isolates Total 8 7 15
Gram () isolates Alfa-hemolytic streptococcus 1 1 2
Gram () isolates Methicillin-resistant S.aureus 0 1 1
Gram () isolates Methicillin-susceptible S.aureus 1 3 4
Gram () isolates Methicillin-sensitive Coagulase (-) Staphylococcus 7 6 13
Gram () isolates Methicillin-resistant Coagulase (-) Staphylococcus 0 2 2
Gram () isolates Corynebacterium spp. 3 2 5
Gram () isolates Total 12 15 27
Fungus Candida albicans 0 1 1
TOTAL 20 23 43
Methods
- This study was designed as a multicenter,
prospective randomized trial. - Patients complying with following inclusion
criteria were included in the study - Neutropenia accompanying hematologic malignancy
or solid tumors (PMNL lt500/mm3) - Fever due to infection (a single measurement of
gt38.5 C or at least two measurements of gt38.0
C, 12 hours apart) - Receiving at least 1 g/m2 cytosine arabinoside
(ARA-C) for patients with acute myelocytic
leukemia or any other hematologic malignancy
requiring chemotherapy - Presence of grade II-IV mucositis according to
WHO or NCI classification at the time of febrile
neutropenia for patients with acute leukemia,
solid tumor or bone marrow transplantation - Study Treatments
- The patients were randomized to receive either
vancomycin or teicoplanin in addition to amikacin
and ceftazidime. - Vancomycin administration i.v. ? Slow infusion, 1
g every 12 hours - Teicoplanin administration i.v. ? Loading dose
400 mg at 12-hour intervals for 3 times - Maintenance dose 400 mg/day
- Duration of treatment 521 days.
- Treatment was discontinued when PMNL count
reached gt500/m3, patient becoming afebrile and no
signs of infection remained.
Efficacy Evaluation Response rates and survival
states were similar in teicoplanin and vancomycin
groups and no statistical difference was observed
between them (Log Rank p0.872, p0.761,
respectively). Survival states and response rates
are presented in Figure 1 and 2, respectively.
Safety Evaluation A total of 91 adverse events
(47 in teicoplanin and 44 in vancomycin groups)
in 56 patients were reported during follow-up
period. Most common adverse events were
hypokalemia, eruption, diarrhea, and
hepatotoxicity. Thirteen of the cases died during
and after the study. Drug-related adverse effects
were observed in 24 of 97 patients (24.7) in
teicoplanin group and 32 of 93 patients in
vancomycin group (34.4), with no significant
difference in terms of rate or severity of
adverse events. A total of 6 patients in
vancomycin and 7 patients in teicoplanin group
died during the study period. The reasons of
deaths were infection (4 patients), bleeding (3
patients), bleeding and infection (2 patients),
underlying disease (4 patients).
Conclusion
In conclusion, our results show that
glycopeptides are valuable in the initial
treatment of febrile neutropenic patients at high
risk of Gram-positive bacteraemia. Teicoplanin is
as effective as vancomycin in terms of treatment
response and overall survival rate. Both
antibiotics have acceptable safety profiles.
The changes in the highest level of fever,
leukocyte count, absolute neutrophil count, ECOG
performance score, infection findings, clinical
focus, and microbiological findings were
evaluated. No statistically significant
difference was present between treatment groups
regarding these parameters.
References
- Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown
AE, Calandra T, et al. 2002 guidelines for the
use of antimicrobial agents in neutropenic
patients with cancer. Clin Infect Dis.
200234730. - Cometta A, O. Marchetti O, Calandra T. Empirical
use of anti-Gram-positive antibiotics in febrile
neutropaenic cancer patients with acute
leukaemia. Eur J Cancer 20075 (suppl)23. - Wood MJ. The comparative efficacy and safety of
teicoplanin and vancomycin. J Antimicrob
Chemother. 199637209.
1Ankara University Medical School, Department of
Hematology, Ankara 2Marmara University Medical
School, Department of Infectious Diseases,
Istanbul 3Adnan Menderes University Medical
School, Department of Hematology, Aydin 4Inonu
University Medical School, Department of
Hematology, Malatya 5Suleyman Demirel University
Medical School, Department of Hematology,
Isparta 6Akdeniz University Medical School,
Department of Pediatric Hematology and Oncology,
Antalya 7Ankara Oncology Hospital, Ankara
8Osmangazi University Medical School, Department
of Hematology, Eskisehir 9Hacettepe University
Medical School, Department of Infectious
Diseases, Ankara, Turkey.
Printed by
Recommended
CrystalGraphics Presentations





























