
Craniosynostosis - PowerPoint PPT Presentation
1 / 55
Title:
Craniosynostosis
Description:
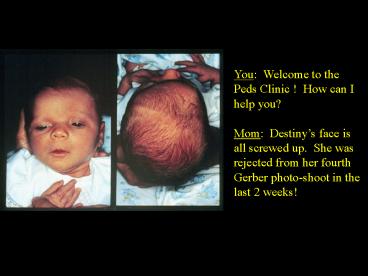
You: Welcome to the Peds Clinic ! How can I help you? Mom: Destiny s face is all screwed up. She was rejected from her fourth Gerber photo-shoot in the last 2 weeks! – PowerPoint PPT presentation
Number of Views:648
Avg rating:3.0/5.0
Title: Craniosynostosis
1
You Welcome to the Peds Clinic ! How can I
help you? Mom Destinys face is all screwed
up. She was rejected from her fourth Gerber
photo-shoot in the last 2 weeks!
2
Normal Infant Skull
Expansile
Flexible
- Flexible enough to get through vagina
- Molding
- Expansile enough to accommodate rapid brain growth
3
(No Transcript)
4
Infant Skull Anatomy
5
Suture Growth
- Sutures allow growth perpendicular to them
- Growth at suture lines related to brain growth
6
Suture Closure
7
Early Closure Causes Growth Parallel to the Suture
8
Craniosynostosis Early Fusion of a Suture
9
(No Transcript)
10
Sagittal Synostosis
Boat-Head (Scaphocephaly)
11
(No Transcript)
12
(No Transcript)
13
Coronal Synostosis
Bent-Head (Plagiocepahly)
14
Right Coronal Synostosis
15
(No Transcript)
16
Metopic Synostosis
Triangle-Head (Trigonocephaly)
17
Metopic Synostosis
18
(No Transcript)
19
Lamboid Synostosis
MATTRESS
Slant-Head (Occipital Plagiocephaly)
20
Isolated Primary Craniosynostosis Sutures Involved
21
Clinical Exam
- OFC
- Head shape (from above, side)
- Ear and facial symmetry
- Palpate suture lines fontanelles
- Look for ridging
- Look for associated anomalies
- Skull X-ray or CT
22
Craniosynostosis
Secondary
Primary
- Microcephaly
- Prematurity
- VP Shunting
- Positioning
Isolated Abnormal Suture Syndromic
23
Prematurity
- Deformational Scaphocephaly
- Impaired mobility prolonged positioning
- Persists until adulthood
- Prevention
- Donut-shaped head supports
- waterbed mattresses
- Does not warrant intervention
24
Former Preemies Head
25
VP Shunting
- Scaphocephaly
- Chronic hydrocephalus thickens the skull
- Once decompression with shunt, the suture fuses
- Surgery Indications
- OFC gt 50 cm (4-5 STDs)
- When VPS performed during when VLBW
26
Microcephaly
- Surgical correction not indicated
- Abnormal OFC
- in primary craniosynostosis, OFC remains normal
yet oddly shaped - Rare cases of multisutural craniosynostosis
restricting head growth, but manifests with
increased ICP
27
PositionalDeformation
- Most common cause
- Usually forehead asymmetry
- Sometimes associated with torticollis
- Usually acts on coronal or lamboidal suture
- 40 of newborns
28
An Epidemic of Lamboidal Plagiocephaly
- 1992 Back to Sleep
- Campaign
- 1996 Tertiary Care
- Centers report rise in
- lamboidal plagiocephaly
- from 3 to 20
29
Sorting out the Epidemic
- 102 Patients with occipital plagiocephaly over 4
year period - Only 4 (3) had true lamboidal synostosis
- The rest were deformational
- Only 3 were progressive (required surgery)
- Other responded to positioning or helmets
30
(No Transcript)
31
(No Transcript)
32
Syndromic Craniosynostosis
- 10-20 of cases
- Autosomal Dominant
- Linked to Chromosome 10q
- Multi-sutural, complex cases
If a suture is fused, check hands, feet, big toe
and thumb
33
Distinguishing Clinical Features in the
Craniosynostosis Syndromes
Muenke Crouzon Jackson-Weiss Apert Pfeiffer Bear-Stevenson
Thumbs Normal Normal Fused to fingers Broad, deviated Normal
Hands Carpal fusion Normal Variable Bone syndactyly Variable brachydactyly Normal
Great Toes Broad Normal Broad, deviated Fused to toes Broad, deviated Normal
Feet Tarsal fusion Normal Abnormal tarsals Bone syndactyly Variable brachydactyly Normal
34
Crouzons
- Normal intellect
- Normal extremities
- 5 have acanthosis nigricans
- 30 have progressive hydrocephalus
35
ApertsCrouzons with Hand Involvement
- Varying intellect (50 with MR)
- Mitten Glove Syndactyly
- Cervical vertebral anomalies
- Rare hydrocephalus
36
Apert Extremity Findings
37
True Craniosynostosis Surgery
- Single Suture Synostosis Confirm by exam and
skull x-rays - Complex cases CT or 3D CT
- X-Ray Fused sutures have a broad ridge of
overgrowth of solid bone along a previous suture,
or suture is completely obliterated - Ridge is especially characteristic of fused
sagittal suture
38
Management
- Surgery vs. Conservative Management
39
The Decision to Operate
- Raised ICP in 1/3 of cases, but no neuro
impairment - Cosmetic considerations usually most important
- affects peer acceptance, parent-child bonding,
self-image and coping
40
Imaging
- Skull X-ray
- CT
- 3-D CT
41
(No Transcript)
42
Surgery
- If not part of syndrome, the earlier the
operation the better - At the latest 6-12 months (by 12 months, skull is
85 of adult size) - For coronal suture, operate before 2 months
because of facial symmetry and visual system
development - Procedure depends on continuing skull growth
- Hospitalization for 3-10 days
43
Surgery
- Syndromic cases may need special airway support
- Blood loss significant due to scalp vascularity
- transfusion rates 20-500 of infant estimated
blood volume - PICU stay (facial edema)
- Results on xray within several days
44
(No Transcript)
45
(No Transcript)
46
(No Transcript)
47
Metopic Synostosis
48
Surgery
- Unilateral coronal suture difficult. Orbital
relocation as well. - Syndromic or multi-suture cases staged repairs.
49
Apert Post-Op
50
CrouzonSurgical Pics
51
Conservative Therapy for Deformational
Plagiocephaly
- Re-positioning
- If no improvement
- by 6 months.
- Helmet Molding
52
Custom Made for each head 24/7 wear for 4 months
53
Ocular Morbidity
- Pre- and post-op impairments seen with unilateral
coronal and metopic synostoses - dossociated movements
- amblyopia
- refractive errors
- Ophtho involvement in work-up and follow-up
54
Long Term Follow-Up
- Speech
- Genetic Counseling
- Feeding / Swallowing
- Ophtho
55
(No Transcript)
Recommended
CrystalGraphics Presentations





























