
Leukocoria - PowerPoint PPT Presentation
1 / 37
Title:
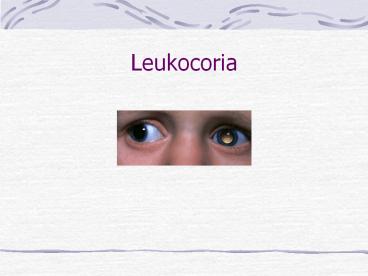
Leukocoria
Description:
Nontraumatic unilateral cataracts first detected after 6 months of age also ... response to the single infection nematode, which must usually be dead before ... – PowerPoint PPT presentation
Number of Views:1386
Avg rating:3.0/5.0
Title: Leukocoria
1
Leukocoria
2
Causes of Leukocoria
- DIFFERENTIAL DIAGNOSIS OF LEUKOCORIA
- Cataract
- Retinoblastoma
- Toxocariasis
- Coats disease
- ROP
- PHPV
- Retinal detachment
- Coloboma
- Retinal dysplasia
- Norries disease
3
Developmental Cataracts
- Nontraumatic unilateral cataracts first detected
after 6 months of age also present special
concerns.Usually, the precise age of onset is not
known. In some cases, particularly those
associated with thinning of the posterior lens
capsule (posterior lenticonus or lentiglobus),
the duration of significant visual deprivation
may have been relatively brief. A history of
recent-onset strabismus or leukocoria,
preservation of good alignment with central
steady fixation (even on a light), family
photographs documenting symmetrical red fundus
reflexes, or pediatrician's records of red reflex
observation can help to establish a good visual
prognosis.
4
Retinoblastoma
- Retinoblastoma is the most common intraocular
tumor of childhood, accounting for 1 of
childhood cancer deaths in the United States and
5 of blindness in children. The incidence is 1
in 15,000 to 1 in 20,000 live births. - Overall mortality from retinoblastoma decreased
from 95 a century ago. With modern diagnostic
and therapeutic advances, the mortality rate from
metastatic or recurrent retinoblastoma has been
as low as 5.
5
RETINOBLASTOMA
- CLINICAL
- MANIFESTATIONS
- Leukocoria (60)
- Strabismus (20)
- OTHER- Uveitis, Orbital cellulitis, Hyphaema,
Heterochromia, Glaucoma, Bupthalmos
6
RETINOBLASTOMA
7
Retinoblastoma
- The disease is bilateral in approximately 30 of
cases. The average age at diagnosis is 18 months
and 90 of patients are diagnosed before the age
of 3 years. Less than 10 of retinoblastoma
suffers have a family history of the disorder,
90 of cases are sporadic. Of the sporadic cases,
the responsible mutation is in a germ cell in
25 of cases and in a somatic cell in 75 of
cases
8
GENETICS
- Retinoblastoma gene is a recessive oncogene of
180,000 kilobases. - Located chromosome- 13q14
- Knudson two hit hypothesis-
- Germinal cells have one defective and one normal
RB gene. - A somatic mutation results in loss of the normal
RB gene and hence retinoblastoma develops
(somatic mutations occur frequently enough in the
developing retina, therefore lesions usually
affect both eyes) - In addition, the first child of a parent who had
had a unilateral retinoblastoma has a 4 chance
of developing the disease
9
(No Transcript)
10
PATHOLOGY
- Arise in primitive photoreceptor
cells.Characteristic histology - Retinoblastomas are composed of poorly
differentiated neuroblastic cells with scanty
cytoplasm and prominent basophilic nuclei. - The tumour proliferates rapidly, with a tendency
to outgrow its blood supply and undergo
spontaneous necrosis. Necrotic tumour being
eosinophilic stain pink. - Characteristic Flexner-Wintersteiner rosettes
represent an attempt at retinal differentiation.
Histologically, a ring of cuboidal cells is seen
surrounding a central lumen. Cuboidal tumour
cells with basally oriented nuclei arranged
around a central lumen. - Calcification is another feature of
retinoblastomas, usually occurring in necrotic
areas. Calcium stains with HE. It is worth
identifying calcium in suspect eyes by
ultrasound, or CT scan to differentiate
retinoblastomas from other tumours.
11
PATHOLOGY
12
Retinoblastoma
13
MANAGEMENT
- EMPIRICAL GENETIC COUNSELLING
- ENUCLEATION
- unilateral, poor visual prognosis
- PLAQUE
- 4-12mm /- vitreous seeding
- EXTERNAL BEAM
- gt12mm, multiple foci, only eye
- LASER
- consider- indirect, xenon arc
- cryotherapy if lt2dd in size
- CHEMOTHERAPY, if intracranial extension
14
Non-Retinoblastoma Malignancies
- Unfortunately, children who have genetic
retinoblastoma and survive their primary
intraocular cancer have a substantially increased
risk of death from one or more nonretinoblastoma
malignancies over the course of their lifetimes,
up to 35 of children who have had a bliateral
retinoblastoma and external beam radiation
therapy will develop a second cancer by age 25
years
15
Congenital retinal telangiectasis (Coats' disease)
- Congenital retinal telangiectasis (Coats'
disease) is an idiopathic retinal vascular
disorder that usually affects young male patients
unilaterally in their first or second decade of
life. Congenital retinal telangiectasis, however,
can affect patients of either gender and become
manifest at any age. Up to one third of patients
are older than 30 years of age at the time of
presentation.There is no defined familial
inheritance. Patients may present with decreased
vision, as well as strabismus or leukocoria in
children. The hallmark feature of congenital
retinal telangiectasis is localized fusiform
aneurysmal dilations of the retinal vessels
reminiscent of tiny light bulbs
16
(No Transcript)
17
Retinal vascular anomalies
- The vascular anomalies can occur anywhere in the
fundus and may involve the capillaries, arteries,
and veins. - Other findings may include vascular loops and
beading, retinal neovascularization, hemorrhagic
retinal macrocysts, and segmentally dilated
capillaries. - Leakage from the incompetent vasculature may lead
to retinal edema, lipid deposition, or, in severe
cases, an exudative retinal detachment. - The extent of retinal involvement is variable.
- Infants and children often are more severely
affected with extensive vascular involvement and
massive subretinal lipid exudate.
18
Persistent hyperplastic primary vitreous (PHPV)
- Persistent hyperplastic primary vitreous (PHPV)
is a congenital anomaly in which the primary
vitreous fails to regress in utero. Highly
vascular mesenchymal tissue nurtures the
developing lens during intrauterine life. In
PHPV, the mesenchymal tissue forms a mass behind
the lens. - A gray-yellow retrolental membrane may produce
leukocoria, with the subsequent suspicion of
retinoblastoma. - In PHPV, the globe is white and slightly
microphthalmic. Patients have no history of
prematurity or oxygen administration.
19
RETINOPATHY OF PREMATURITY (ROP)
- Vasoproliferative retinopathy affecting premature
infants exposed to high oxygen - INCIDENCE
- Prematurity (lt32/40)
- Birth weight (30 lt 1000gm affected)
- Oxygen duration
- 90 ROP regresses spontaneously, 5 blindness
20
RETINOPATHY OF PREMATURITY (ROP)
- In the early active stages of ROP, a band of
glomeruloid capillaries proliferates at the
junction between the peripheral nonperfused and
the posterior perfused retina. The proliferating
vessels break through the internal limiting
membrane and invade the vitreous, inciting
fibrosis and contraction. In the later
cicatricial stages of ROP, the retina is folded
on itself by the organized vitreous, forming a
fibroneural mass that drags the macula and optic
disc temporally. The end stage of the disease is
marked by total retinal detachment, leukocoria,
blindness, and phthisis bulbi.
21
RETINOPATHY OF PREMATURITY (ROP)
- LOCATION
- zone 1 - centred on disc, 2x disc to fovea
distance - zone 2 - outer limit equator temporally, ora
nasally - zone 3 - temporal peripheral crescent
- in clock hoursrush disease- SI-SV in 2/52
- CLASSIFICATION - STAGING
- SI- flat demarcation line with branching blood
vessels up to line - SII- ridge with volume, blood vessels enter ridge
- SIII- ridge extraretinal fibrovascular
proliferation - SIV- retinal detachment- a (not involving the
fovea), b (involving the fovea) - SV- total RD, open or closed funnel
- plus disease- dilated tortuous vessels in
posterior pole, vitreous haze and poor mydriasis
22
RETINOPATHY OF PREMATURITY (ROP)
- LOCATION
- zone 1 - centred on disc, 2x disc to fovea
distance - zone 2 - outer limit equator temporally, ora
nasally - zone 3 - temporal peripheral crescent
23
(No Transcript)
24
RETINOPATHY OF PREMATURITY (ROP)
25
Toxoplasmosis
- Toxoplasmosis gondii is an obligate intracellular
protozoa causing up to 50 of cases of posterior
uveitis. - Ocular infection is characterised by focal
necrotising retinochoroiditis with vitritis.In
congenital infection the eye may also be affected
by cataract, microphthalmos, and optic atrophy
26
Chorioretinitis and congenital toxoplasmosis
- The main clinical manifestations of the
symptomatic form of toxoplasmosis are
microcephaly or hydrocephaly, cerebral palsy,
epilepsy, mental retardation, cerebral
calcification, and chorioretinitis. - The most important signs in the diagnosis of
congenital toxoplasmosis are the three Cs
convulsions, calcification (intracranial), and
chorioretinitis. Chorioretinitis is present in
80 of children with congenital toxoplasmosis and
is most often bilateral toxoplasmosis is
considered one of the most common causes of
chorioretinitis.
27
Congenital Toxoplasmosis
- Highest transmission occurs in the IIIrd
trimester - 90 of congenital infections have no clinical
signs - Earlier infection occurs in pregnancy - worse
potential outcome - Triad- convulsions,
- cerebral calcification
- and chorioretinitis
- Eye - chorioretinitis, cataracts, microphthalmos,
panuveitis, optic atrophy
28
Investigation of Toxoplasmosis
- ELISA IgM in neonates, rising IgG in adults
(although not that helpful in adults). - Fluorescein angiography (hypofluorescence in the
early stages and then progressive leakage). - Indocyanine angiography - multiple small dark
spots may be seen around the visible lesions
implying the affected retina is greater than
apparent initially. This sign may be useful in
assessing the effect of treatment.
29
Some indications for active treatment of
toxoplasmosis
- Lesions that involve the macula, papillomacular
bundle or optic disc - Large, active lesions should be treated.
- Immunocompromised patients should be treated.
30
Ocular toxocariasis
- Ocular toxocariasis is a unilateral disorder that
presents as strabismus, leukocoria or decreased
vision. Retinal damage is the result of the
host's inflammatory response to the single
infection nematode, which must usually be dead
before the uveitis can develop. The posterior
uveitis may be of severe intensity.
31
Toxocariasis subretinal granuloma
- Ocular toxocariasis may present with decreased
vision, strabismus, leukocoria, or uveitis. - Most commonly a subretinal granuloma is present
in the posterior pole in an otherwise quiet eye. - In the early stages, it is elevated above the
retina and may resemble a neoplasm.
32
Retinal detachment in childhood
- Retinal detachment in childhood can be confused
with retinoblastoma, and vice versa. The
possibility of an underlying retinoblastoma
should always be considered when a child presents
with retinal detachment and vitreous hemorrhage,
even when a history of trauma is obtained.
Appropriate preoperative studies (ultrasonography
or computed tomography) are indicated if
vitrectomy is performed, the specimen should be
submitted for cytologic examination.
33
Retinal detachment in childhood
- Retinal detachment in childhood can be confused
with retinoblastoma, and vice versa. The
possibility of an underlying retinoblastoma
should always be considered when a child presents
with retinal detachment and vitreous hemorrhage,
even when a history of trauma is obtained.
34
Norrie disease
- Norrie disease, or the progressive
oculoacousticocerebral degeneration of Norrie, is
a rare, X-linked recessive heritable disorder
characterized by bilateral leukocoria caused by
retinal detachment. Affected boys classically
have a triad of blindness, deafness, and mental
retardation. Apparent at birth or in early
infancy, the ocular findings usually progress to
phthisis bulbi. An identical disorder in a
Maltese kindred is called Episkopi blindness.
35
Retinal dysplasia
- Retinal dysplasia and PHPV are characteristic
ocular findings in trisomy 13 in fact, trisomy
13 was called retinal dysplasia before the
chromosomal defect was identified. The multitude
of systemic and ocular findings found in patients
with trisomy 13 may include bilateral leukocoria.
Rarely, retinal dysplasia occurs unilaterally in
the congenitally malformed eyes of otherwise
healthy persons.
36
COLOBOMA
- OPTIC DISC COLOBOMA
- Due to failure of closure of foetal fissure
inferiorly - May be isolated disc or associated chorioretinal
coloboma - ISOLATED DISC COLOBOMA
- Rare,
- Usually sporadic, some AD
- Can be bilateral
- Visual acuity varies from normal to NPL.
- Associated- optic disc pit, hyaloid artery
remnant, myopia, posterior lenticonus,transphenoid
al encephalocoele, cardiac defects, VII palsy - RETINOCHOROIDAL COLOBOMA
- ASOCIATIONS
- Coloboma of iris, aniridia, PHPV, microphthalmos
- Associated CVS, CNS and ear malformations
37
CHARGE !
- CHARGE (For diagnosis at least 4 of the
highlighted abnormalities are required). - Colobomas,
- Heart defects,
- Choanal Atresia,
- Retarded growth,
- Genital abnormalities,
- Ear abnormalities
- CHARGE is also associated with facial palsy,
micrognathia, cleft palate, pharyngeal
incompetence, tracheo-oesophageal fistula, renal
and cardiac abnormalities. - Note many other syndromes have colobomata.