
Corynebacterium - PowerPoint PPT Presentation
1 / 21
Title:
Corynebacterium
Description:
Corynebacterium C. diphtheriae: causes diphtheria. Other corynebacteria (coryneform) may cause opportunistic infections. Gram-positive, irregularly-shaped rod. – PowerPoint PPT presentation
Number of Views:1256
Avg rating:3.0/5.0
Title: Corynebacterium
1
Corynebacterium
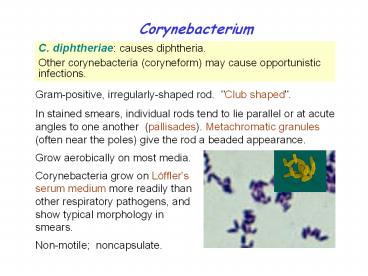
C. diphtheriae causes diphtheria. Other
corynebacteria (coryneform) may cause
opportunistic infections.
Gram-positive, irregularly-shaped rod. "Club
shaped". In stained smears, individual rods tend
to lie parallel or at acute angles to one another
(pallisades). Metachromatic granules (often near
the poles) give the rod a beaded appearance.
Grow aerobically on most media. Corynebacteria
grow on Löffler's serum medium more readily than
other respiratory pathogens, and show typical
morphology in smears. Non-motile noncapsulate.
2
C. diphtheriae
Pathogenesis and Immunity C. diphtheriae occurs
in the respiratory tract, in wounds, or on the
skin of infected persons or normal carriers. It
is spread by droplets or by direct
contact. Portal of entry respiratory tract or
skin abrasions. Diphtheria bacilli colonize and
grow on mucous membranes, and start to produce
toxin, which is then absorbed into the mucous
membranes, and even spread by the
bloodstream. Local toxigenic effects elicit
inflammatory response and necrosis of the faucial
mucosa cells-- formation of "pseudo-membrane
(composed of bacteria, lymphocytes, plasma cells,
fibrin, and dead cells), causing respiratory
obstruction. Systemic toxigenic effects necrosis
in heart muscle, liver, kidneys and adrenals.
Also produces neural damage.
3
C. diphtheriae
Clinical Diseases
Respiratory diphtheria Incubation period 2-6
days. Inflammation begins in the respiratory
tract, causing sore throat, exudative pharyngitis
that develops into pseudomembrane, and low grade
fever. Prostration and dyspnea????? ????? soon
follow, which may lead to suffocation if not
promptly relieved by intubation or
tracheotomy. Damage to the heart causes irregular
cardiac rhythm. Visual disturbance, difficulty in
swallowing and paralysis of the arms and legs
also occur but usually resolve spontaneously.
Death may be due to asphyxia or heart failure.
Cutaneous diphtheria mild (papule ulcer
with grayish membrane) with little toxigenic
effects. Stimulates antitoxin production.
4
C. diphtheriae
Laboratory Diagnosis
Specific treatment should be given before the lab
reports if the clinical picture strongly suggests
diphtheria. Specimens swabs from the nose,
throat or suspected lesions. Gram's stain beaded
rods in typical arrangement (unreliable). Culture
inoculate specimen onto a blood plate, a Löffler
slant, and a tellurite plate. Identification
biochemical tests. Toxigenicity test 1. in vivo
test inject the culture into antitoxin-protected
and unprotected guinea pigs subcutaneously. 2.
Tissue culture neutralization assay. 3. in
vitro test immunodiffusion assay (Elek test
). 4. Detection of toxin gene by PCR.
5
C. diphtheriae
Treatment
Treatment of diphtheria rests on prompt
administration of antibiotics (penicillin,
erythromycin) and diphtheria antitoxin. Maintenanc
e of an open airway. Treatment of bacteremia or
endocarditis must be guided by antibiotic
susceptibility tests.
6
C. diphtheriae
Prevention and Control
Humans are the only known reservoir of C.
diphtheriae. Diphtheria was mainly a disease of
small children. This organism is maintained in
the oroparynx or skin of asymptomatic carriers.
The bacteria are spread directly from person to
person. To limit contact with diphtheria
bacilli to a minimum, patients with diphtheria
should be isolated. Prophylactic antibiotic
treatment to unimmunized contacts.
7
C. diphtheriae
Prevention and Control
Active immunization in childhood with diphtheria
toxoid yields antitoxin levels adequate until
adulthood. All children must receive an initial
course of immunizations and boosters. Regular
booster with Td (tetanus and diphtheria) toxoids
are particularly important for adults who travel
to developing countries. Schick test can be used
to test susceptibility of a person to diphtheria.
Toxoids for delayed absorption Fluid toxoid
absorbed onto aluminum hydroxide or aluminum
phosphate. Usually combined with tetanus toxoid
and/or pertussis vaccine (DPT vaccine).
8
Other Corynebacterium Species
They are ubiquitous in plants and animals. Many
are found as part of human normal flora and may
cause opportunistic infections, such as
pneumonia, endocarditis, and soft tissue and bone
infections, in immunocompromised patients. C.
jeikeium sepsis, endocarditis, wound infections,
foreign body infections. C. urealyticum causes
UT infections. It is a strong urease producer,
infection of UT may lead to formation of
stones. C. ulcerans is closely related to C.
diphtheriae. May cause diphtheria-like
disease. Resistant to many antibiotics. Treatment
of bacteremia or endocarditis must be guided by
antibiotic susceptibility tests.
9
Listeria and Erysipelothrix
L. monocytogenes meningitis and bacteremia E.
rhusiopathiae erysipeloid
Structure and Physiology Small gram-positive
coccobacilli, facultative anaerobic. Motile at
room temperature but not at 37 oC. Grow on most
conventional media in a wide pH range and cold
temperatures.
10
L. monocytogenes
Pathogenesis and Immunity Widely distributed in
nature (soil, water, vegetation, and the
intestines of a variety of animals). Fecal
carriage in healthy people 1-5. Human disease
is restricted to neonates and the elderly,
pregnant women, and immunocompromised patients
(particularly those with defective cell-mediated
immunity, such as AIDS patients). Facultative
intracellular pathogen. The intracellular
survival and spread of the bacteria are
critically important in pathogenesis and,
therefore, cellular immunity is more important
than humoral immunity in host defense against
this organism.
11
L. monocytogenes
Clinical Diseases
Adults Healthy Asymptomatic or mild
influenza-like illness. Gastrointestinal
symptoms in some patients. Immunocompromised Meni
ngitis (high risk organ transplant patients,
cancer patients, pregnant women) Primary
bacteremia chills and fever high fever and
hypotension in severe cases. Maybe fatal.
Neonates Early onset disease (acquired
transplacentally in utero) granulomatosis
infantiseptica, with disseminated abscesses and
granulomas in multiple organs. Late onset disease
(acquired at or soon after birth) meningitis or
meningoencephalitis with septicemia, similar to
that caused by group B streptococci.
12
L. monocytogenes
Laboratory Diagnosis Specimen CSF and
blood. Gram stain CSF typically show no Listeria
because of the low bacterial concentration. Cultur
e Listeria grows on most conventional
media. Selective media and cold enrichment are
used for specimens contaminated with rapidly
growing bacteria. Hemolysis (b-) and motility in
liquid or semisolid medium are useful for
preliminary identification. Identification Bioche
mical and serological tests.
13
L. monocytogenes
Treatment, Prevention, and Control L.
monocytogenes is resistant to multiple
antibiotics (e.g., cephalosporin and
tetracycline). Currently, penicillin or
ampicillin, either alone or with gentamicin, is
the treatment of choice. Outbreaks have been
associated with the consumption of contaminated
milk, soft cheese, undercooked meat, unwashed raw
vegetables, and cabbage. Refrigeration of
contaminated food products permits the slow
multiplication of the organisms to an infectious
dose. Because Listeria organisms are ubiquitous
and most infections are sporadic, prevention and
control are difficult. High risk people should
avoid eating raw or partially cooked foods.
14
Erysipelothrix (Hair of red disease)
E. rhusiopathiae Slender gram-positive,
microaerophilic, with a tendency to form
filaments. Form small, grayish a-hemolytic
colonies after 2 to 3 days incubation. Widely
distributed in wild and domestic animals. Animal
disease (particularly in swine) is widely
recognized, but human disease is uncommon.
Causes zoonotic infections through an abrasion
or wound Localized skin infection
(erysipeloid) 1-4 day incubation painful and
pruritic, slowly spreading inflammatory skin
lesions on the fingers or hands, violaceous with
raised edge. Suppuration is uncommon. Generalize
d (diffuse) cutaneous infection rare and often
associated with systemic manifestation. Septicem
ia uncommon and frequently associated with
endocarditis.
15
Erysipelothrix
Penicillin is the antibiotic of choice. Specimen
full-thickness biopsy specimens or deep aspirates
(because the bacteria locate only on deep
tissues). Culture grow on most conventional
media in the presence of 5-10
CO2. Identification Motility- and
catalase-negative. Biochemical tests. People at
occupational risk (butchers, meat processors,
farmers, poultry workers, fish handlers, and
veterinarians) are prevented by use of gloves and
other coverings on exposed skin. Vaccination is
used to control disease in swine.
16
(No Transcript)
17
Diphtheria toxin is an A-B toxin expressed from a
temperate phage (b-phage) in the presence of low
iron concentrations. This toxin binds to
receptors on the surface of many eukaryotic
cells, particularly heart and nerve cells, and
results in inhibition of polypeptide chain
elongation by ribosylation of the elongation
factor EF-2. It can induce protective antibodies
(antitoxin).
Back
18
Bull-neck appearance???? ??? ??
Back
19
Back
20
Internalins
Listeriolysin O
ActA
Back
21
(No Transcript)
Recommended
CrystalGraphics Presentations





























