
60x36 Poster Template - PowerPoint PPT Presentation
1 / 1
Title:
60x36 Poster Template
Description:
Non-authorized printing of this poster template by any commercial printing service other than PosterPresentations.com is strictly prohibited. Non-profit educational ... – PowerPoint PPT presentation
Number of Views:217
Avg rating:3.0/5.0
Title: 60x36 Poster Template
1
An Atypical Presentation of Odontalgia in a Child
with Down Syndrome A Case Report.
Shaun Gabriel, MD, Sean Smith, MD, Joseph
Hornyak, MD, PhD University of Michigan Health
System, Department of Physical Medicine and
Rehabilitation. Ann Arbor, Michigan
ABSTRACT
BACKGROUND
Patient A 9-year-old girl with Down Syndrome and
progressive acute onset neck pain. Case
Description The patient presented with a history
of several months of intermittent progressive
cervical pain after an unwitnessed fall from her
bed. She was seen at an urgent care center 2-3
days later with complaints of neck and shoulder
pain, however, physical exam and plain
radiographs were negative. Her pain progressed
and localized to her neck, and she was
subsequently seen in the emergency room twice for
her pain, but again, exam and imaging were
negative. Flexion/extension spine films did not
demonstrate instability or fracture, and cervical
MRI showed no evidence of cervical instability or
spinal cord compression. She had occasional
relief with NSAIDs and was referred to the
pediatric PMR clinic for further
evaluation. Results One week prior to her clinic
appointment with her pediatric physiatrist, the
patients primary deciduous tooth was replaced by
her permanent tooth and she had complete
resolution of her cervical pain. On physical
exam, she presented with decreased tone,
hypermobility and features consistent with Down
Syndrome, but her exam was otherwise unremarkable
without reproduction of pain over her cervical
spine, shoulders or paracervical musculature. Her
cervical range of motion was full and there was
also no evidence of periodontal pain, pulpal
pain, facial neuralgia, arthromyalgia, or TMJ or
muscles of mastication pain. Discussion Atypical
Odontalgia (AO) is a condition that entails
hyperesthesia and increased sensitivity of a
tooth or group of teeth without evidence of
pathology on exam or imaging. Pain typically
includes a continuous burning or aching pain in
the tooth, bone, or gums that can spread to the
face, neck, and shoulders. To our knowledge,
however, this case is the first documented
instance of AO presenting as referred cervical
pain without complaint of primary odontalgia.
Other potential pathologies are TMJ disorder and
myofascial pain, yet these conditions often
include face, neck and shoulder pain, with rare
limitation to the tooth, which was not seen in
this patient on repeat examinations. It is
possible that she had difficulty expressing her
pain location appropriately. Conclusion This
case demonstrates that cervical pain in the
pediatric population may be referred pain from
odontalgia. Atypical odontalgia can include the
neck and shoulders, and in the pediatric
population with developmental delay disorders,
workup for dental pain should be included for
appropriate diagnosis and treatment.
Atypical Odontalgia (AO) is atypical facial pain
related to apparently normal teeth. Symptoms
generally include hyperesthesia with burning and
aching sensations in the teeth, gums, and/or
bone. Pain can radiate to the jaw, face, neck,
and other areas, is typically constant, and often
times follows invasive dental procedures.
Graff-Radford and Solberg diagnostic criteria
include 1. Continuous or almost continuous pain
in a tooth or alveolar bone, 2. Pain present for
more than four months, 3. No obvious local cause,
4. Normal radiographs, 5. No evidence of referred
pain, 6. Diagnostic nerve pain is equivocal.1
Though AO is typically found in women in their
40s, it can affect all demographics.
Deafferentation appears to be the cause of the
pain, but psychological factors and alteration of
neural mechanisms seem to play a role as well.
2 Neck pain in Down Syndrome (DS) can be a
serious issue. About 13 of DS patients are at
increased risk of excessive mobility/instability
of the occiput and atlas (C1), or the axis (C2)
and atlas.3 This excessive mobility may lead to
spinal cord compression, symptoms of which can
include neck pain, weakness, headache, and
torticollis.
2. DISCUSSION
1. CASE PRESENTATION
Atypical Odontalgia (AO) is a
hyperaesthetic condition that usually manifests
as a constant burning and/or aching sensation in
a tooth, teeth, gums, and/or bone. The pain can
radiate to the neck, head, and shoulders. The
pain is predominantly at the original site in the
dentition. To our knowledge, this is the first
reported case of AO manifesting as neck pain
without an original or concurrent complaint of
dental pain. In a patient with Down
Syndrome, neck pain is a potential emergency,
especially in the setting of possible trauma,
which is the case with the patient that we
present. Part of the work-up should include
cervical spine imaging (X-rays and perhaps an
MRI) and a detailed physical exam. Atlantoaxial
instability should be in the differential, and
symptoms can include pain and neurologic
deficits, such as weakness. It is
entirely possible that this patient was not able
to localize her pain to her parent and
physicians, making the diagnosis more difficult.
A detailed history should be obtained, including
history of trauma, recent dental procedures, and,
in the case of the pediatric population, status
of primary versus permanent teeth.
Normally, the treatment for AO involves as-needed
non-opiod pain medications, such as ibuprofen.
Given possible underlying neural dysfunction as a
cause, tricyclic antidepressants or
anticonvulsants are often prescribed for
treatment, though topical medications such as
capsaicin are effective in many cases. 4 As with
any clinical condition, however, identifying the
underlying cause in this case the growth of a
permanent tooth under a primary is the most
important factor in deciding treatment.
The patient is a 9-year old female who
was seen in the pediatric PMR clinic for an
approximate 2-month history of constant,
progressive neck pain. It was initially
discovered when her mother was at an urgent care
center for her own medical issues, and the
patient complained of neck pain and stated that
she had fallen out of bed. X-rays taken at
urgent care were negative for fracture or
subluxation. Her pain was initially
intermittent but became constant, affecting her
both at school and at home, and with no temporal
attributes. She was seen in the ER twice, and
flexion/extension films were again negative for
any acute process, including signs of
atlanto-axial or atlanto-occipital instability.
The pain progressed to the point where it would
cause her to cry, and was debilitating. She took
ibuprofen as needed which provided occasional
relief. MRI of the neck showed no evidence of
spinal cord or root compression. The
patients mother then reported that a week before
her visit to the pediatrics PMR clinic, one of
the patients primary teeth spontaneously came
out and a permanent tooth was in its place. The
patients neck pain resolved shortly after the
passing of her primary tooth and did not recur.
Neurological and musculoskeletal exams were
unremarkable at the clinic visit except for some
joint hypermobility, though her cervical spine
range of motion was within normal limits. On
review, the impacted tooth can be seen on MRI.
At a three-month follow-up visit, her pain
remained absent with no intermittent recurrences.
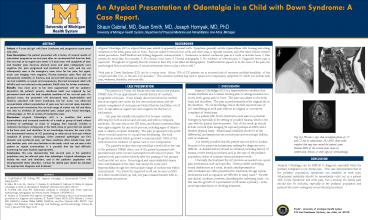
Top (L) Flexion x-rays show incomplete fusion of
C1 and C2 but no subluxation. (R) MRI shows
tooth eruption that may have caused the patients
pain. Bottom MRI of the cervical spine shows
no compression, stenosis, or other signs of cord
pathology.
CONCLUSION
Atypical Odontalgia can be difficult to diagnose,
especially when the primary complaint is not
dental pain. This case demonstrates that in the
pediatric population, symptoms can manifest as
neck pain. Atlantoaxial instability should be
immediately ruled out in a patient with Down
Syndrome and neck pain, but a workup for dental
pain should also be included, especially in the
pediatric population and patients who have
undergone recent dental procedures.
REFERENCES
1. Graff-Radford SB, Solberg WK. Atypical
odontalgia. J Craniomandib Disord. 1992
Fall6(4)260-5. 2. Melis, M, Lobo SL, Ceneviz,
C, Zawawi, K, Al-Badawi E, Maloney G, Mehta N.
Atypical odontalgia a review of the literature.
Headache. 2003 Nov-Dec43(10)1060-74. 3.
Pueschel SM, Scola FH. Atlantoaxial instability
in individuals with Down syndrome epidemiologic,
radiographic, and clinical studies. Pediatrics.
198780(4)555. 4. Analysis of 50 patients with
atypical odontalgia A preliminary report on
pharmacological procedures for diagnosis and
treatment. E. Russell Vickers MDSc, BDS, Michael
J. Cousins MD, FANZCA, Suellen Walker MBBS,
FANZCA, and Ken Chisholm MD, FRCPC. Oral Surgery,
Oral Medicine, Oral Pathology, Oral Radiology,
and Endodontology, Volume 85, Issue 1, January
1998, Pages 24-32.
PMR - University of Michigan Health System 325
East Eisenhower Parkway, Ann Arbor, MI 48108
Recommended
CrystalGraphics Presentations





























