
LSUHSC - PowerPoint PPT Presentation
1 / 22
Title: LSUHSC
1
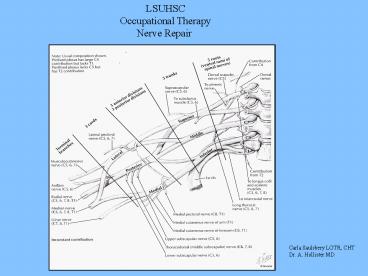
LSUHSC Occupational Therapy Nerve Repair
Carla Saulsbery LOTR, CHT Dr. A. Hollister MD
2
Nerve Repairs Primary nerve repair
Indicated for clean, sharply cut nerves.
Performed immediately after an injury or
within 1 to 2 weeks Secondary nerve repair
Usually indicated in the presence of a severely
crushed or avulsed nerve Appropriate post
operative immobilization is important. The
expected rate of recovery for nerve repairs is 1
inch per month, after an initial period of 3
weeks when the axonal sprouts cross the
repair Patient must be educated, especially with
an insensate hand Care must be taken to avoid
stretching of the repaired nerve ends. Tension
leads to scarring Motor retraining, sensory
reeducation and desensitization programs should
be initiated as sensory and muscle
reinnervation becomes evident
3
Median and Ulnar Nerve Repair Surgeon dictates
wrist position in the OR. A dorsal plaster
Kleinert splint applied 0-3 weeks post
repair OT fabricates a thermoplastic Kleinert
dorsal blocking splint. Same wrist position
as placed in OR. If associated Flexor Tendon
repair follow FTR protocol for splinting and PROM
If lesion is more proximal include a long arm
splint with the elbow flexed to 90º If no tendon
injury begin AROM/AAROM to digits Educate
patient on insensate areas. ADL
adaptations Monitor for thumb adduction
contracture with Median nerve injury Begin scar
massage once wound is healed 3 weeks post
repair A volar wrist splint is molded with wrist
in neutral OT performs baseline Semmes and motor
examination. Assess Tinels Assess grip and
pinch (wait until week 6 with tendon
injury) AROM exercises Patient education on
insensate hand Cocoa butter massage to hand for
hydration, desensitization and massage to scar
4
4 weeks post repair Patient education on the
expected sensations associated during
sensory return Serial splint the wrist into
extension weekly. Check for complaints of
burning and tingling during extension of the
wrist while forming splint Decrease extension
and mold splint prior to this point Massage to
entire hand for skin re-hydration The hand
should be kept warm during cold weather.
Patient should use glove or tube sock for
warmth. Continue patient education on insensate
hand. Use of visual compensation Continue AROM
exercises. Continue PROM with associated tendon
repair Assess Tinels. Document location 5
weeks post repair Lumbrical bar can be added to
the volar wrist splint for Ulnar nerve
lesion Continue AROM exercises. Continue PROM
with associated tendon injury Continue patient
education on insensate hand Massage for
desensitization, skin re-hydration AROM
exercises to the wrist
5
6 weeks post repair Volar wrist splint is
discontinued Lumbrical bar splint for ulnar
nerve lesion C-bar splint and or opponens splint
for median nerve lesion Re-evaluate sensation
and motor exam. Assess grip and pinch Begin
sensory reeducation and desensitization program
when appropriate Continue education on insensate
areas ?Assess Tinelss 7-8 weeks Dynamic
splinting can begin for ulnar nerve to improve
extrinsic flexor tightness Continue with
Lumbrical bar for Ulnar nerve and opponens for
Median nerve 6-12 weeks post repair Motor
retraining as appropriate OT repeats sensory and
motor examinations every 3 to 4 weeks. Continue
to assess for Tinels. Document
Tinels Functional activities Strengthening Con
tinue sensory reeducation Continue splinting as
indicated
6
Median nerve innervation
Ulnar nerve innervation
7
Lumbrical bar splint Ulnar Nerve
Dynamic splint for ulnar nerve injury
8
Short opponens for Median Nerve
C-bar for correction of a thumb adduction
contracture
9
Median Nerve Deficits (wrist level) Sensory loss
of the central palm area and the palmar surfaces
of the lateral three and one-half
digits Weak MCP joint flexion of the index and
middle fingers due to paralysis of the first
two lumbricals Weak pinch due to paralysis of
opponens pollicis. abd. pollicis brevis, and
the superficial head of the flexor pollicis
brevis Loss of palmar abduction due to
paralysis of the APB Anterior Interosseous Nerve
(AIN) (Proximal 1/3rd of forearm) Loss of DIP
joint flexion of the index and middle fingers due
to paralysis of the FDP to each digit Loss
of thumb IP flexion due to paralysis of the
flexor pollicis longus (FPL) Weak forearm
pronation due to paralysis of the pronator
quadratus Median Nerve lesion in the proximal
forearm Weak forearm pronation due to paralysis
of the pronator teres Weak wrist flexion due to
paralysis of the flexor carpi radialis
(FCR) Weak finger flexion due to paralysis of
the flexor digitorum superficialis (FDS)
10
Median Nerve C6-T1 MMS Pronator Teres
Forearm Median Nerve
High Lesion Flexor Carpi Radialis
Palmaris Longus
Flexor Dig. Superficialis Flexor Dig
Profundus(IF/LF)
Anterior Interrosseous Flexor Pollicis
Longus Pronator Quadratus
Abd. Poll. Brevis Hand
Median Nerve Low Lesion
Opponens Pollicis Flexor Pollicis
Brevis Lumbricals (1,2)
11
Ulnar Nerve lesion at the wrist Loss of
abduction and adduction due to paralysis of the
interossei Hyperextension of the ring and small
MCP joints with flexion of the IP joints due
to unopposed action of the extensor digitorum
communis (EDC) and the flexion of the flexor
digitorum profundus Weak thumb adduction due to
paralysis of the adductor pollicis Loss of
opposition of the fifth finger due to paralysis
of the abd. digiti quinti Weak thumb opposition
due to paralysis of the AdP Weak MCP flexion due
to paralysis of the third and fourth
lumbricals Weak pinch due to paralysis of the
AdP, deep head of the FPB and the first
dorsal interosseous Weak grasp due to paralysis
of the interossei, third and fourth lumbricals,
and the FDP of the ring and small
fingers Sensory loss of the volar and dorsal
aspects of the medial third of the hand, the
small finger and the ulnar half of the ring
finger Ulnar Nerve lesions in proximal forearm
involves these additional problems Weak flexion
of IP joints of the ring and small fingers due to
paralysis of the ulnar half of the FDP Weak
wrist flexion due to paralysis of the flexor
carpi ulnaris (FCU)
12
Ulnar Nerve C8-T1 MMS Flexor Carpi Ulnaris
Forearm
High Lesion Flexor Dig.
Profundus(RF/SF) Abd. Digiti Minimi
Hand
Low Lesion Opponens Digiti Minimi
Flexor Digiti Minimi
Lumbricals 3,4 Interossei
(palmar/dorsal) Flexor Pollicis
Brevis (deep) Adductor pollicis
Froments Thumb IP flexion during lateral
pinch Positive Froments in hand B
13
Radial Nerve repair Patient is placed in volar
plaster post op splint by Surgeon in OR 0-3
weeks post repair OT fabricates a volar forearm
based static wrist extension splint. Wrist
extended 60º. If lesion is more proximal the
elbow should also be immobilized in 90º of elbow
flexion. Dynamic finger extension outriggers
may be added AROM /AAROM of the digits ?With
associated extensor tendon repairs follow
splinting protocol for zone of injury.
Patient education in ADL modifications ?Patient
education in wound care progressing to scar
massage 3-6 weeks post repair Volar wrist
splint is molded with wrist in 45º of
extension Dynamic finger extension outriggers
are added to daytime splint A volar wrist cock
up splint is fabricated for night-time wear OT
performs baseline motor and sensory evaluation.
Assess Tinels Assess grip and pinch strengths
at 6 weeks ADL modifications as needed Check
for Tinels. Document advancement
14
Long arm splint for more proximal Radial nerve
injury
15
Radial Nerve Repair 6-12 weeks post
repair Continue with splinting as indicated for
positioning and function Continue to monitor
motor return Begin motor retraining when
appropriate ?Continue to re-assess sensation,
grip, pinch and MMS ?Assess Tinels. Continue to
document advancement ?Continue to advance ADLs
16
Radial nerve motor innervation
17
High Radial Nerve lesion wrist drop due to
paralysis of wrist extensors Diminished
abduction and extension of the thumb due to
paralysis of the abductor pollicis longus (APL)
and the extensor pollicis brevis (EPB) Inability
to extend MCP joints due to paralysis of the long
extensors Weak grasp and pinch due to
inefficiency of the unopposed flexors Loss of
sensation of the lateral two thirds of the dorsum
of the hand, a portion of the dorsum of the
thumb and the dorsum of the proximal phalanges
of the lateral three and one-half
digits Weakened supination due to paralysis of
the supinator muscle Posterior Interosseous
Nerve Lesion Same effects as described except
sensation is not lost and wrist extension is
present but weakened.
18
Radial Nerve C6, 7, 8 and T1 MMS Triceps
Radial Nerve
High Lesion
Brachioradials Wrist Extension
ECRL
ECRB Posterior Interosseous
Supinator
Posterior Interosseous Low Lesion
Ext. Digitorum Ext. Digiti
Minimi Ext. Carpi Ulnaris
Abd. Pollicis Longus Ext.
Pollicis Longus Ext. Pollicis
Brevis Ext. Indicis Proprius
19
Splinting for Radial Nerve
Volar wrist splint Begin with wrist extension at
60 and Serial splint towards neutral
Dynamic splint, no active wrist extension
Dynamic Splint, Active wrist extension
20
Volar
Dorsal
Semmes Weinstein
21
Digital Nerve Week 1 post op Dorsal Blocking
Kleinert splint. MCPs flexed 60º and IPs in
full extension AROM exercises within splint 15
reps hourly Wound Care Weeks 1-3 post
op Dorsal Blocking Kleinert splint AROM
exercises Scar massage Patient education on
insensate area Baseline Semmes Weinstein Weeks
3-6 post op AROM exercises Scar
massage Desensitization/sensory
re-education Begin ADLs ?Tinels ?Patient
education on insensate areas
22
Digital Nerve Weeks 6-8 post op Repeat Semmes
Weinstein Extension splinting as needed for
flexion contracture Continue patient education
on insensate areas Continue desensitization Week
8-10 post op Strengthening ?Repeat Semmes
Weinstein ?Assess Tinels ?Continue
desensitization/sensory re-education
Recommended
CrystalGraphics Presentations





























