
Peripheral Vascular Disease - PowerPoint PPT Presentation
1 / 55
Title:
Peripheral Vascular Disease
Description:
Do not wear garters or knee stockings. Do not swim or wade in cold water. ... wear elastic stockings. Elevate legs for at least 20 minutes 4-5 x daily ... – PowerPoint PPT presentation
Number of Views:6183
Avg rating:3.0/5.0
Title: Peripheral Vascular Disease
1
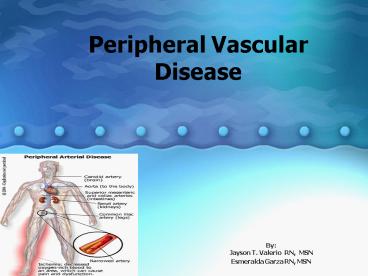
Peripheral Vascular Disease
- ByJayson T. Valerio RN, MSN
- Esmeralda Garza RN, MSN
2
Peripheral Vascular Disease
- is a term used to describe a group of diseases
that involve a pathophysiological changes in the
peripheral arteries or veins resulting in blood
flow disturbances. - Peripheral Arterial Disease - is the most common
cause of PVD - 2 Types of PAD
- Organic
- Functional
- Chojnowski, D (2005). Peripheral Arterial
Disease. Nursing made Incredibly Easy!, 4 (3),
4-17
3
2 Types of Arterial Disease
- Acute Arterial Insufficiency
- involves a complete blockage, sudden in onset and
constitutes an emergency treatment. - Chronic Arterial Insufficiency
- - slow in onset, common cause is atherosclerosis,
one limb is usually affected more than the other.
4
Epidemiology, Incidence and Prevalence
- PAD affects 12-20 percent of Americans age 65 and
older (8-10 million) - By 2050 the prevalence could reach 9.6-16 million
among those age 65 and older and 19 million
overall - According to National Heart, Lung and Blood
Institute and the American Heart Association
(AHA), the cost of cardiovascular disease in 2003
was estimated 352 billion. - Black Americans appear to be affected more often
than white Americans or Hispanics - PAD generally occurs in men older than 45 years
of age and in post menopausal women
5
Etiology
- Atherosoclerosis main cause
- Risks
- Hypertension
- Hyperlipidemia
- DM
- Cigarette smoking
- Obesity
- Familial predisposition
- Advancing age
- High level of homocysteine
- Cardiovascular disease
- Cerebrovascular disease
- Stress
- Diet
- Male gender
6
PAD indicator of systemic disease
- PAD is a strong indicator of systemic
atherosclerotic disease. Related to coronary
artery disease, which affects up to 60 of the
patients with PAD, and cerebrovascular disease,
which affects between 40 to 50 of the patients
with PAD.
7
Enlarged View of Atherosclerosis
8
Pathophysiology
- Cause Atherosclerosis and Risk factors
- Partial or total arterial obstruction
- Diminish blood supply
- Deprivation of oxygen and nutrients
- Vessel wall injury
- Accumulation of fatty substance
- Tissue dies
PAIN
9
Signs and Symptoms
- Pain Intermittent Claudication
- pain triggered by exercise one
block - Rest pain(Usually 2to5 minutes)
- Loss of hair
- Dry, scaly, dusky, pale and mottled skin
- thickened toe nails
- Cold, gray or darkened extremity
- Pallor-when elevated
- Rubor when dependent
- Diminish or absent peripheral pulses
- Paresthesias
10
Signs and Symptoms
- Pain in calf, buttock, thigh or foot
- My aching legs
- Feeling cramping, muscle tightness, fatigue, and
aching in lower legs. - Hip or legs giving out
- Cant walk very far
11
Chronic PAD
- Stage I Asymptomatic
- No claudication is present
- Pedal pulses decreased
- Stage II Claudication
- Muscle pain, cramping and burning with exercise
relieved with rest - Symptoms reproducible with exercise
12
Chronic PAD
- Stage III Rest Pain
- Pain while resting awaken at night
- Pain distal portion of the ext.
- Pain is relieved by placing the ext. in a
dependent position - Stage IV Necrosis gangrene
- Ulcers/blackened tissue in toes
- Gangrenous odor present.
13
Diagnostic Tests
- X-ray arteriography of the legs
- Segmental systolic BP measurements
- Exercise Tolerance Testing
- Plethysmography
14
Plethysmography
15
Medical Management Non Surgical
Exercise Positioning Promoting vasodilation Drug
therapy Percutaneous Transluminal
Angioplasty Laser-Assisted Angioplasty Atherectomy
Surgical Revascularization
16
Angioplasty
17
Medical Surgical Management
- Surgical treatment
- Arterial Revascularization has two
classifications - a.1. Inflow procedures involve bypassing of
arterial occlusions above the superficial femoral
arteries (SFAs) - Ex aortoiliac, aortofemoral, axillofemoral
- a.2. Outflow procedures involve bypassing of
arterial occlusions at or below the SFAs. - Ex femoropopliteal, femoropopliteal
18
An axillofemoral bypass graft
Aortoiliac and aortofemoral bypass
surgerymidline incision
19
Management Arterial Revasularization
- Pre-operative Care
- general care for pre-op
- with emphasis on v/s, peripheral pulses
- Post-operative Care
- assessment of graft occlusion
- promotion of graft patency
- treatment of graft occlusion
- monitor for compartment syndrome
- assessment of infection
20
Nursing Management Plan of Care Chronic
Pain Ineffective Tissue Perfusion
Peripheral Risk for Injury Risk for Peripheral
Neurovascular Dysfunction
21
Nursing Management
- Assess the extremities for peripheral pulses,
pain, color, temperature and capillary refill at
least every 4 hours as needed. - Assess clients level of pain at least q 4 hrs or
prn - Keep extremities warm using lightweight blankets,
socks and slippers. - Encourage the client to change position at least
every 2 hours. - Avoid crossing legs and restrictive clothing.
22
Assessment Scale Peripheral pulses
- 0absent
- 1diminished
- 2normal
- 3increased
- 4bounding
23
Nursing Management
- f. Teach methods to prevent further injury
- Obtain proper foot care and nail care
- Reduce stress
- Stop smoking
- Prevent exposure to extreme heat or cold
- Avoid extended pressure on your feet and ankles
- HESI HINT!!! Decreased blood flow results in
diminished sensation in the lower extremities.
Any heat source can cause severe burns before the
client actually realizes the damage is being done.
24
Foot care for the client with PAD
- Wash legs and feet daily in warm water using mild
soap - Pat dry using soft towel, dry in between toes
- Use powder on the feet and between the toes
- Buy shoes in the afternoon
- Wear clean pair of socks each day
- Wear shoes or slippers when getting out of bed
- Walk on level ground
- Do not go barefoot.
25
Foot care
- Inspect legs and feet daily with mirror
- Have professional foot care provider
- Always check temperature of water
- Do not sunburn top of legs
- Report foot and leg problems promptly
- Do not cross legs
- Do not wear garters or knee stockings
- Do not swim or wade in cold water.
26
Peripheral Venous Disease
- 2 Primary categories
- Occlusive Venous Disorders
- life threatening
- Ex. Venous thrombosis (thrombophlebitis and deep
vein thrombosis) - 2. Defective valves
- are not life threatening but are problematic
- Ex. Varicose veins
27
- Thrombophlebitis refers to a blood clot that is
associated with inflammation. This can occur in
superficial veins however it can frequently occur
in the deep veins of the lower extremities (deep
vein thrombophlebitis or deep vein thrombosis) - Phlebothrombosis is a thrombus without
inflammation
28
Deep Vein Thrombosis (DVT)
- is a blood clot that usually forms in the deep
veins of the calf or the proximal veins of the
leg. - is more common and poses a life threatening
because it presents a greater risk for pulmonary
embolism (PE).
29
Etiology of DVT
- Unknown
- Risk Factors
- Certain surgical procedures
- Over 40 years old
- Pregnancy
- Ulcerative Colitis
- HF
- Immobility
- Phlebitis
- Severe infections
- Oral Contraceptives
- Trauma
- Malignancy
30
Epidemiology, Incidence and Prevalence
- According to American Heart Association, up to
2.5 million Americans are affected annually by
DVT. - It is estimated that 50,000-100,000 individuals
die each year of PE. - Black individuals have a high rate of death
resulting from PE.
31
Health Promotion and Illness Prevention
- Avoid oral contraceptives
- Drink adequate fluids
- Exercise legs during periods of prolonged bedrest
or sitting - Client education
- Early ambulation
- Use of graduated compression stockings
- Use of sequential compression device
- venous plexus foot pump
32
Pathophysiology of DVT
- In 1856, Rudolph Virchow identified 3 factors
that contribute to the formation of thrombus
leading to DVT. - 1. Venous stasis
- 2. Vessel wall injury
- 3. Hypercoagubility
33
Signs and Symptoms CLASSIC Calf or groin
tenderness Pain Sudden onset of unilateral
swelling of the leg
34
Diagnostic
- Physical examination
- Venography
- Duplex Ultrasonographic Scanning
- Impedance plethysmography
- D-dimer test
- VQ Scan
- Complications of DVT
- Pulmonary embolism
35
Medical Management
- Non-surgical
- Rest and elevation of extremity
- Drug of Choice anticoagulants
- . Heparin (IV)
- . Low molecular weight heparin (LMWHs)
- . Warfarin therapy
- . Thrombolytic therapy
- Surgical
- Thrombectomy
- Inferior vena caval interruption
36
An inferior vena caval (IVC) filter
37
Nursing Management Plan of Care Risk for
Ineffective Tissue Perfusion Peripheral Acute
Pain
38
Nursing Care
- Assess clients level of pain on regular basis
- Asses peripheral pulses, skin integrity,
capillary refill and color of extremities once
per shift - Measure the diameter of the calf and thigh of
the affected extremity upon admission and daily
thereafter - d. Maintain bed rest and elevate extremities at
all times. - e. Maintain use of ordered antiembolic
stockings. - Encourage position changes at least q 2 hours
- g. Administer and monitor the effectiveness of
analgesics, antibiotics, thrombolytic and
anticoagulant therapy.
39
Venous Insufficiency
- occurs as a result of prolonged venous
hypertension which stretches the veins and
damages the valves. - Epidemiology, Incidence and Prevalence
- The prevalence rate varies from 0.6 to 1.6 per
1000 for adults and increases up to 10-30 per
1000 in persons older than 85 years of age. - Between 1.9-2.5 billion yearly is spent on
venous disease in the USA
40
Clinical Manifestations
- may have edema in both extremities
- discoloration of ankle (stasis dermatitis)
extending up to the calf - ulcers often form typically over the malleolus
more often medially than laterally and usually
have irregular borders
41
(No Transcript)
42
Medical Management
- Objectives To heal the ulcer and prevent stasis
with recurrence of ulcer formation. - Treatment of Edema
- wear elastic stockings
- Elevate legs for at least 20 minutes 4-5 x daily
- Avoid prolong sitting and standing in place
- Use of sequential compression device as ordered
43
- Treatment of Venous Stasis Ulcers
- Use of occlusive dressings such as oxygen
permeable dressing and oxygen impermeable
hydrocolloid dressing such as duoderm - Application of Unna boot if client is ambulatory
- Drug therapy use of topical agent such as
accuzyme use of systemic antibiotics
44
Arterial vs Venous
45
Arterial vs Venous
46
Aneurysms
- is a sac formed by dilation of an artery
secondary to weakness and stretching of the
arterial wall.
47
Etiology
- Atherosclerosis with hypertension
- Smoking
- Syphillis
- Syndromes
- Marfan
- Ehlers-Dahlos
48
Types of Aneurysms
- Fusiform a diffuse dilation affecting the
entire circumference of the artery. - Dissecting separation of the arterial wall
layers to form a cavity that fills with blood.
- Saccular an outpouching affecting only a
distinct portion of the artery.
49
- Abdominal Aortic Aneurysm
- Mostly saccular or dissecting
- Severe to mid lower abdominal pain
- Low back pain
- Mass in periumbilical area
- Bruits heard over the mass
- Pulsating abdominal mass
- Diminish femoral pulse
- Occurs in men over
- 50 Years old
- Caused by
- Atherosclerosis
- HTN
- Trauma
- Infection
- Thoracic Aortic Aneurysm
- Diffuse and deep chest pain
- Hoarseness of the voice
- Dysphagia
- Dyspnea
- Distended neck veins
- Edema of the head and arms
50
Diagnostic Assessment
- Aortography or X-ray
- Computed tomographic (CT Scan)
- Ultrasonography
- Medical Surgical Management
- Note depends on the size of the aneurysm and
presence of symptoms - Non surgical management
- control of hypertension
51
Surgical Management
- AAA
- abdominal aortic aneurysm
- extracorporeal circulation is not needed
- Thoracic Abdominal Aneurysm
- thoracic aortic aneurysm repair
- extracorporeal circulation is needed
52
Surgical Management Pre-operative
- Type anesthesia General
- Obtain a signed consent
- NPO post midnight
- IV line
- Indwelling catheter
- Blood typing and cross matching
- Obtain Vital signs
- Check peripheral pulses
53
Intraoperative
- AAA resection
- expect a midline abdominal incision from the
xiphoid process to the symphysis pubis or a wide
transverse incision from flank to flank
- Thoracic aortic aneurysm repair
- - thoracotomy or strenotomy
54
Postoperative Care
- Critical Phase 24-48 hours
- Note for common post-op complications such as
- MI
- Graft occlusion
- Hypovolemia/Hemorrhage/Renal failure
- Respiratory distress
- Paralytic ileus
- Paraplegia
55
Discharge Plan Home Care/Rehabilitation Facility
- Health teachings
- A. Non surgical client
- s/s of AAA and thoracic aortic aneurysm
- diagnostic and MD follow up regularly
- B. Surgical Client
- avoid lifting heavy object 15-20 lbs for 6-12
weeks - Avoid activities that are strenuous and increase
thoracic/abdominal pressure - Constant MD and diagnostic follow up
- Signs and symptoms of wound infection
Recommended
CrystalGraphics Presentations





























